Thursday, May 25, 2006
major ed concerns
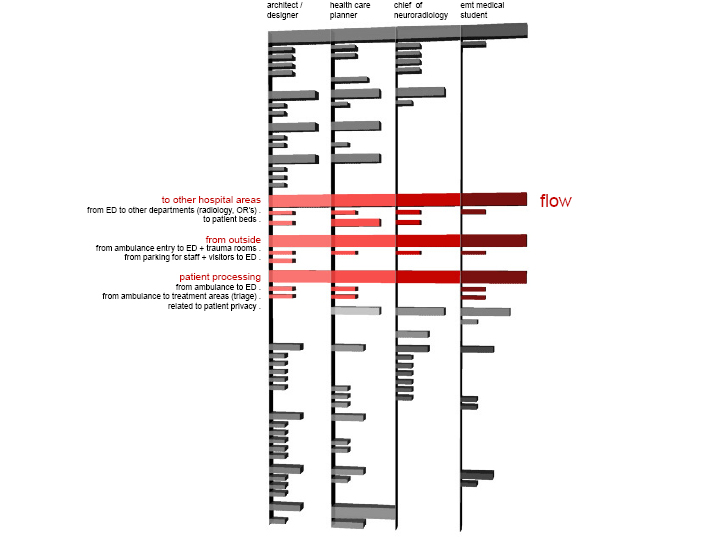
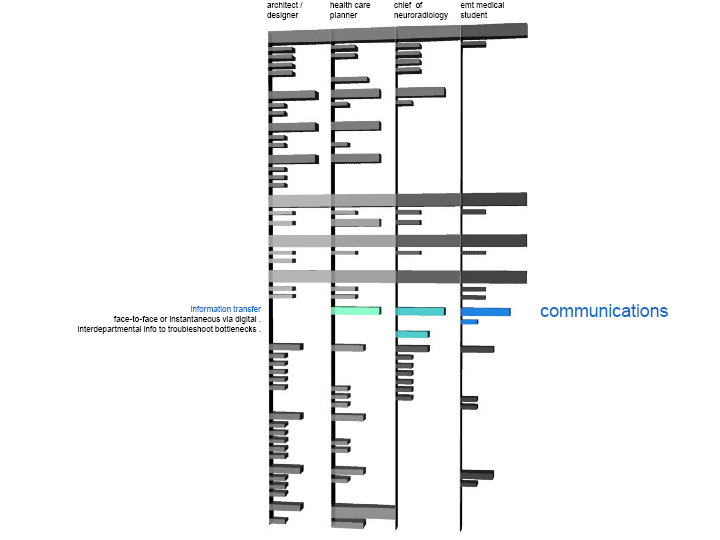
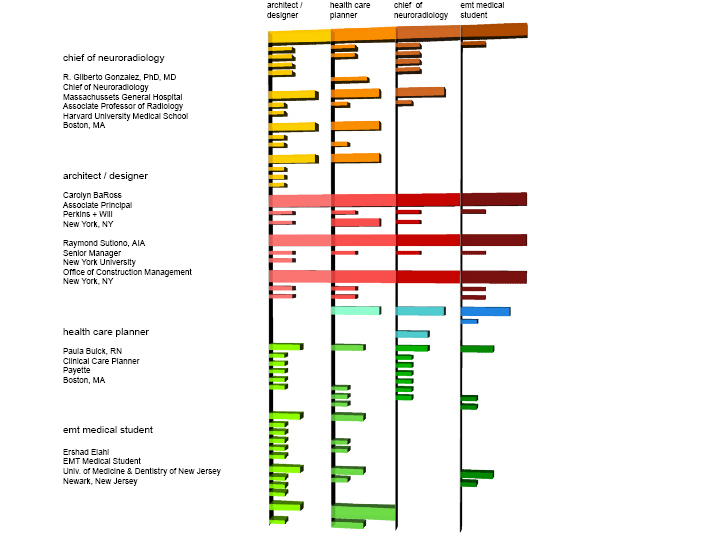
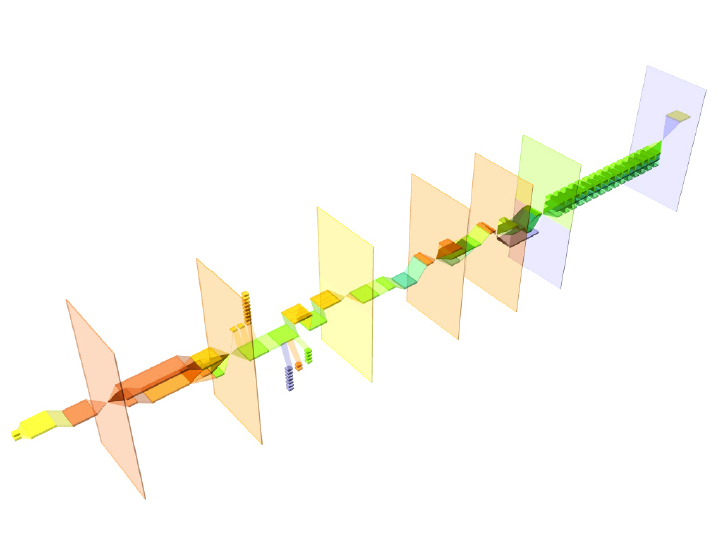
hi again. here are the images for the major concerns of the ED according to various people.slide 1:

slide 2:

slide 3:
slide 4:
slide 5:

slide 6:
sharon at 1:24 AM
Wednesday, May 24, 2006
construction process - final
so..... the different parts of the process didn't change in size, etc. but the staging and explanation of the process did become clearer with the following sequences of images. and the length of the boxes do correlate with time in relation to each other.overall:
stage one - hospital administrative

stage 2: design development process
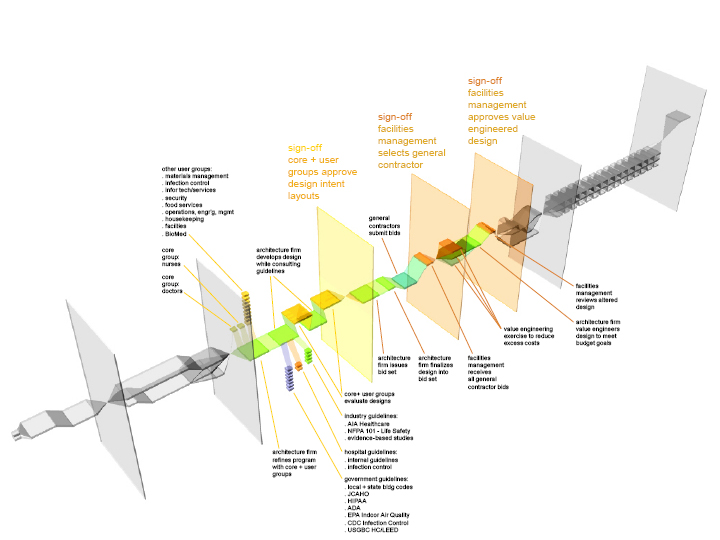
stage 3: construction process and move-in

s.
sharon at 7:51 PM
Monday, May 22, 2006
construction process - part 2
hello again...in an attempt to stick with the 3D view of the construction process, here are two versions
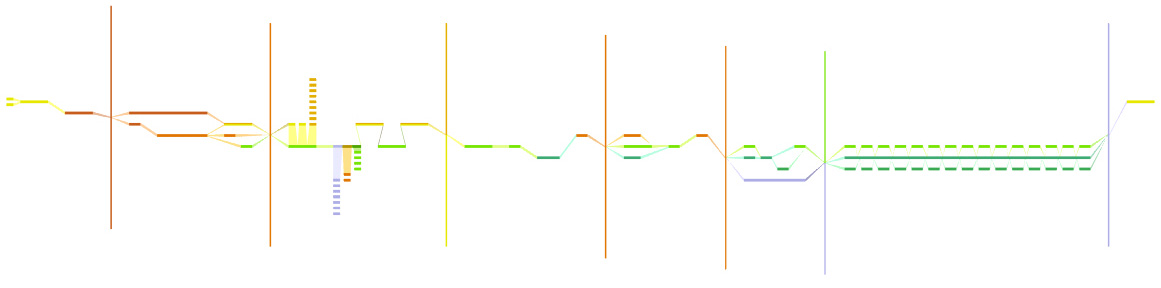
the first one uses really thin lines to represent the stages that require a signature before the process can proceed... not so effective:
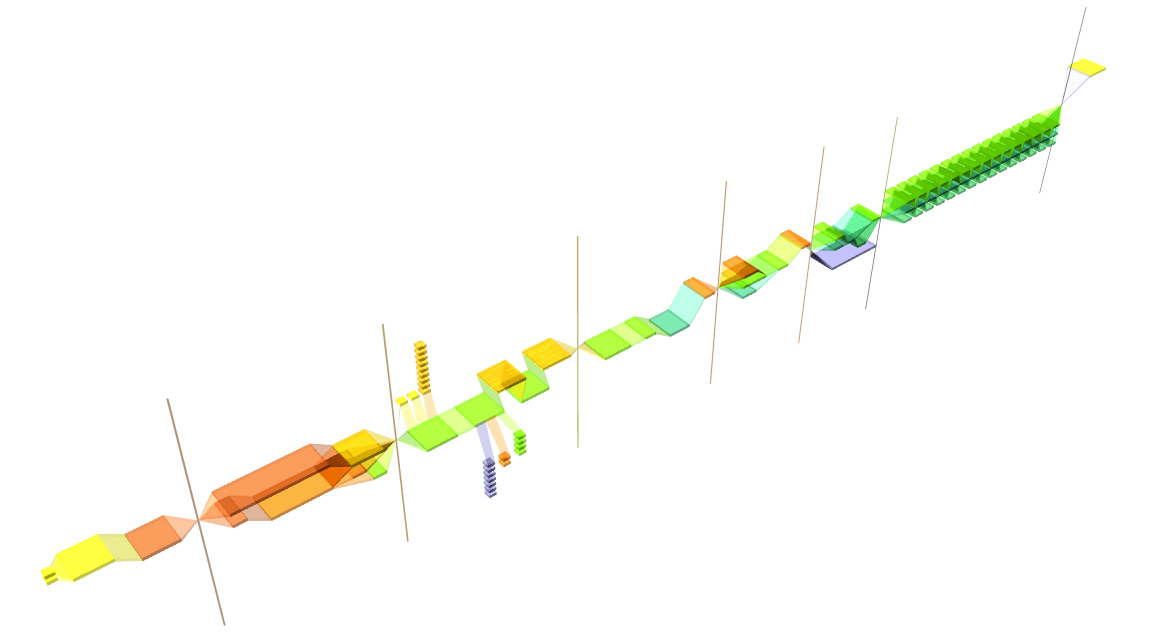
then i tried it using a suggestion from irwin - clearer planes with darker edges. shows the blocking of the process a little better:

comments??
also, i know that the different parts need to get fatter/skinner to correlate with its importance in relation to the other parts. that'll get done soon afterwards.
s.
sharon at 8:33 AM
Wednesday, May 17, 2006
clearer representation of the construction process?
hey guys,i did some revisions on the construction process diagram. it's not as fancy to look at, but it probably shows the process more clearly. there are two versions that i'd like your feedback on.
the first one is a slightly 3D view...

the second one is just a flat view...
so, votes on which one to proceed with?
thanks, sharon
{kind=link}
sharon at 10:30 PM
Tuesday, May 16, 2006
Transportation to th ER
-Boston MedFlight (BMF) is a CAMTS accredited Critical Care Transport service- 3 helicopters,
- Fixed wing aircraft
- 2 critical care ground vehicles.
-BMF's mission is to extend the tertiary care services of the major Boston hospitals to the citizens of Massachusetts and New England, 24/7
-Non profit organization, BMF transports patients regardless of their ability to pay.
-MedFlight is financially supported in part by a consortium of Boston hospitals including Beth Israel Deaconess Medical Center, Boston Medical Center, Brigham and Women's Hospital, Children's Hospital, Massachusetts General Hospital, and Tufts New England Medical Center.
-Established 1985
How does BMF decide which vehicle is most appropriate on interfacility transport requests?
Decision
Most appropriate vehicle to the requested hospital based on safe and efficient transportation.
Normally decided by Communications Specialists in conjunction with the BMF Medical Crew.
BMF online Medical Control is available to discuss vehicle selection with referring/receiving physicians and BMF staff.
Mission completion
1. Safety
If the helicopter is requested, the pilot must accept/reject the mission.
If helicopter transport cannot be completed safely, BMF will offer the hospital BMF's ground critical care unit or fixed wing jet service, if appropriate and available. Advantages = same crew configuration and same medical equipment.
Disadvantage = longer wait time on the part of the sending facility.
2. Patient Condition
If the patient is in need of emergent services unavailable at the sending facility, such as a cardiac catheterization lab or an operating room, BMF will triage the request to the helicopter flight team.
If the patient requires nonemergent transport, such as transport to a hospital for elective procedures, and is being maintained on therapies beyond the scope of ALS providers, BMF will triage this request to the ground critical care unit or fixed wing jet, if available and appropriate. This allows for appropriate utilization of resources by enabling the helicopter to be available for time sensitive requests.
3. Location
Long distance transfer outside of helicopter range will be triaged to fixed wing jet services.
Capable of traveling 1400 miles without refueling
Less affected by weather considerations.
In instances where travel is required outside of the immediate Boston area, fixed wing jet services provide expedited and economical transport between facilities.
Anonymous at 8:41 AM
MGH ER analysis 3
MGH-Massachusetts General Hospital (MGH), incorporated in 1811
-Third oldest voluntary, not-for-profit hospital in the United States
-Oldest in New England.
-Bed capacity approximately 900
-More than 37,000 patients are admitted every year.
-MGH is the original teaching hospital of Harvard Medical School
-Named in the top three hospitals in the United States by US News and World Report for the past several years.
MGH ER
- Full-service, state-of-the-art ED facility
- Provides care for over 75,000 patients annually.
- About a quarter of ED patients are admitted to the hospital.
- Acute Unit of 11 beds 4 shock-trauma resuscitation rooms
2 burn resuscitation rooms
4 cardiac acute care beds
- Major Multipurpose area
17 bays for acute adult illness.
- 4-bed Pediatric Unit
- 10-bed Minor Surgery Unit for walk-in patients.
- 7 bed Rapid Diagnostic Unit (RDU) for patients with single system acute illness.
- Acute Psychiatry Service (APS)
- Emergency Radiology Suite
3 radiology exam rooms
ultrasound suite
2 dedicated multi-detector helical CT scanners
dedicated ED MRI
All ED radiologic images are handled electronically and can be accessed within the clinical areas by computer.
2 portable bedside ultrasound devices used for trauma and acute resuscitations.
- Access to the hyperbaric chamber in the Massachusetts Eye and Ear Infirmary
- Full-weather heliport on the roof of the Blake Building allows two helicopters to access the institution simultaneously
- Frequent destination for Boston MedFlight, a multi-hospital consortium program providing air and ground critical care transport in New England and beyond, utilizing three helicopters, a CitationJet fixed-wing aircraft, and a ground critical care vehicle.
- Level I Trauma Center, Level I Pediatric Trauma Center, Level I Burn Center.
- Only hospital in the United States to hold all three designations simultaneously.
- One of the busiest Level I Trauma Centers in Massachusetts,
- Internationally recognized tertiary referral center and local city hospital
Reference
http://www.massgeneral.org/ed/ED_aboutus.htm
Anonymous at 8:32 AM
ER Communications: Commerical Solutions
Medical Personnel CommunicationOne interesting platform that I have come across is by MedLink Inc.
(Stud Health Technol Inform. 1999;64:93-107. "MediLink: a wearable telemedicine system for emergency and mobile applications." Koval T, Dudziak M. Medical College of Virginia, Richmond, USA)
Personnel in critical care or emergency situations have different needs from those working in other environments where telemedicine and mobile computing have been tested.
"One constructive criticism of the telemedicine initiative has been to question what positive benefits are gained from videoconferencing, paperless transactions, and online access to patient record."
Medlink offers a multipurpose mobile telemedicine applications, aiming to address the 'architecture' of the problem.
Transpac hardware
- A wearable personal computer with a smart-card interface
- Speech, pen, video input and wireless intranet connectivity.
- Structured and noise-resistant speech-to-text interfacing
- Web browser-like display
- Access through flatpanel, standard, or headset monitor,
- Beltpack TransPAC computer has functions of a complete desktop
- PCMCIA card interfaces for internet connectivity
- Secure smartcard with 16-bit microprocessor and upwards of 64K memory provides user access control for security, user custom configuration of applications and display and vocabulary, and memory to diminish the need for PC-server communications while in an active session.
"The TransPAC system with the MedLink software system is designed to provide an integrated solution for a broad range of health care functions where mobile and hands-free or limited-access systems are preferred or necessary and where the capabilities of other mobile devices are insufficient or inappropriate."
TransPAC is being implemented for EMT and ER staff usage.
Patient Information Control
MedLink also produces an 'Optical Memory Card'
Offers patients a portable, durable, high capacity storage device that can be appended but never erased for storing permanent medical history.
"Presently in use by the by the United States and other world governments, the technology embedded within the MedLink EHR card is highly counterfeit-resistant and tamper-proof, providing physicians and their patients added security and peace of mind."
_. Offers up to 4.1MBytes of digital capability
_. Store up to 1,430 pages of text or up to 465 images
_. Data can be updated thousands of times per card
_. Out performs other plastic material cards on durability & storage
_. Data can be appended, never erased
_. Automatically creates an audit trail of patient record updates & changes
_. Multiple layers of security protect data against unauthorized access
_. Most cost effective data storage card
_. Conforms to Industry Standards for optical memory cards and the Uniform Healthcare Identification Card (ANSI X3.284 1997)
Why Connect the Patient?
instant data entry (immediate admin and billing processing = receivables)
accessible (fewer redundant forms = patient satisfaction)
admin records (accurate data insurance eligibility = billable)
accurate data entry (reduced errors = administration costs)
accessible chart (fewer tests, faster accurate diagnosis = costs)
patient satisfaction (instill loyalty and marketing message to community = market share and revenues)
Reference
http://www.medlinkus.com/services.asp?p=memorycard
Anonymous at 8:02 AM
ER Communications Systems
Emergency Room CommunicationsSynchronous communication (face-to-face or telephone conversations) accounted for almost 90% of communications traffic in one study of ER communications. This brings about problems of inducing clinical errors through disrupted memory process, overloaded short-tem memory because of the combination of interruptions, multitasking, and sheer volume of information that is often unwanted or irrelevant.
Efficacy of communication systems is also a problem: for example, senior personnel expects to be paged twice 'if it really is an emergency', resulting in higher levels of communication, and further time-wasting. Vincent and Wears quote an earlier study, decribing that, "despite their own disinclination to be interrupted, clinicians often initiate communication or request information without any thought of the impact of their request on the other person. This is a form of suboptimisation, in which trying to increase one's own performance results in a net decrement in performance over the entire organization."
Reference
Communication in the Emergency Department: separating the signal from the noise
Charles A Vincent and Robert L Wears
MJA 2002; 176 (9): 409-410
Communication channels in the ER
- Face-to-face
- Telephone
- Pager
- Computer
- Patient's medical record
- Forms
- Medical literature
- Test results
- Drug manual
- Letter
- Whiteboard
Communication Typologies
- Formal communication: When a message conforms to a predetermined structure (ie, is in a predefined form).
- Informal communication: When the message structure is determined solely by the conversing parties.
- Synchronous communication: When two parties exchange messages across a communication channel at the same time (eg, telephone).
- Asynchronous communication: When communication exchange does not require both parties to be active in the conversation at the same time (eg, email). The recipient can deal with communication at a time of his or her choosing.
- Interruption: A communication event in which the subject did not initiate the conversation, and which used a synchronous communication channel.
- Multitasking: A period when two or more concurrent communication events occur.
Reference
Communication loads on clinical staff in the emergency department
Enrico W Coiera, Rohan A Jayasuriya, Jennifer Hardy, Aiveen Bannan and Max E C Thorpe MJA 2002; 176 (9): 415-418
In hospitals, response times are critical and efficacy of staff-to-staff communication and patient-staff communication is vital. What is on offer on the market gives pointers to market demands, which include:
Desirables
- Enabling hospital personnel to remain fully accessible at all times.
- Immediate access
- Not interfering with hospital wireless or electronic devices.
- Easy integration with existing systems
- Single-number solutions that integrates all existing systems and numbers.
Categories
- Hospital televisions - MATV & RF Distribution
- On-demand education/information systems
- Satellite systems - entertainment, teleconferences, and programming packages
- Nurse call systems, intercom and overhead paging
- Infant abduction and patient wandering
- Access control systems
- CCTV surveillance/security systems
- In-building wireless phone systems
- Service and maintenance
Hospital personnel-Patient communication systems
- Constant contact with patient care providers, beginning from the ambulance parking lot, Enabling nursing staff to receive instant text messages through integration with nurse calls systems.
- Allowing the nursing staff to conduct initial assessment of a patient’s needs while consulting with a physician, remotely.
- Enabling the physician to consult with specialists in a ‘hands-free’ mode
- Providing family members of acutely ill patients a way to remain in close contact with hospital staff
- Permitting maintenance and security personnel to receive critical alarm and security notification via text messaging
- Accelerates access to mobile hospital staff via networking of multiple locations
Implements an effective disaster recovery solution that supports and maintains communication.
Reference
Ascom Wireless Solutions (http://www.hospcom.com/Hospcompdfs/04-PRIVATEWIRELESSPHONESYS/01%20-%20TIME%20IS%20CRITICAL.pdf)
Issues/questions?
- Is text messaging as the best means of communication within the ER and between hospital departments?
- How else can we transmit this data in a less cumbersome, more instantanaeous way? Special ER/treatment related symbols on a handset? Conventional video-confereing via cellphone? Are unita by the bedside with hands-free access for instant communication better than pager systems?
Emergency Communication Systems
- Patient emergencies
- Disorderly patients
- Wandering patients
- Code blue teams
- ED
- Chemical/Hazardous material environments
Need
An automatic system to ensure quick response times.
Process
- Automatic / user-initiated control to raise alarm.
- Notification, escalation and routing of distress signals to pre-defined team members .
- Discussion of situation via group call.
o Identify the nature of the emergency situation
o Talk to the initator of the emergency
o Ensure proper equipment and personnel are identified and gathered simultaneously
o Discuss estimated arrival times and team member proximity to emergency
o other team members can be notified by text message
- Reaction: fast and coordinated.
Reference
http://www.hospcom.com/Hospcompdfs/04-PRIVATEWIRELESSPHONESYS/12%20-%20EMERGENCY%20NOTIFICATION%20SOLUTION.pdf
One Australian study attempted to address the problem that few studies of communication between healthcare professionals exist, observing
- Time involved in communication
- number of communication events
- interruptions, and overlapping communications
- choice of communication channel
- purpose of communication
between 12 clinical staff members, comprising six nurses and six doctors in two emergency departments, one 200 bed rural hospital and one 540-bed urban tertiary teaching hospital, in New South Wales hospitals, in 1999.
“5 hours and 13 minutes were observed, and 1286 distinct communication events were identified, representing 36.5 events per person per hour (95% CI, 34.5–38.5). A third of communication events (30.6%) were classified as interruptions, giving a rate of 11.15 interruptions per hour for all subjects; 10% of communication time involved two or more concurrent conversations; and 12.7% of all events involved formal information sources such as patients' medical records. Face-to-face conversation accounted for 82%. While medical staff asked for information slightly less frequently than nursing staff (25.4% v 30.9%), they received information much less frequently (6.6% v 16.2%).
Their conclusion supports the “need for communication training in emergency departments and other similar workplaces. The combination of interruptions and multiple concurrent tasks may produce clinical errors by disrupting memory processes. About 90% of the information transactions observed involved interpersonal exchanges rather than interaction with formal information sources..”
“Several studies quantifying the impact of poor communication on clinical work suggest that communication is a likely cause of systematic error in the health system. In Australia, inadequate communication has been associated with 17% of system problems, and, of these, 84% were deemed potentially preventable.1 About 50% of all adverse events detected by general practitioners were associated with communication difficulties.2 Within intensive care units, 2% of the activity consists of verbal communication between nurses and doctors, but accounts for 37% of error reports.3 Thus, the evidence strongly suggests that poor communication wastes time, threatens patient care and may be one of the chief culprits behind preventable adverse events in clinical practice.4
The research reported here extends work begun in the United Kingdom in the mid-1990s,5,6 in which it was found that physician teams in hospital were subject to high levels of interruption. Clinical staff also appeared to bear a higher communication load than necessary, considering the many tasks that could be accomplished by accessing information sources rather than asking questions of people. It has since been hypothesised that such interruptions impose cognitive loads on clinical staff and have a negative impact on memory, leading to clinical error.7”
The following points I found of most interest:
- Nearly a third of communication events were classified as interruptions,: that they were not initiated by the observed subject, and occurred using a synchronous communication channel such as face-to-face conversation.
- Subjects were carrying out two or more overlapping conversations (multitasking) for 10% of the total communication time.
- About 90% of the information transactions observed involved interpersonal exchanges rather than interaction with formal information sources. (Their conclusion being that this suggests a low upper limit on the potential for electronic medical records (EMRs) to improve information processes within healthcare organizations, since the EMR is essentially a formal medium.)
Purpose of communication events in the emergency department
Communication events are expressed as a proportion of all communication events, by clinical role (NOS = not otherwise specified)
Reference Communication loads on clinical staff in the emergency department
Enrico W Coiera, Rohan A Jayasuriya, Jennifer Hardy, Aiveen Bannan and Max E C Thorpe MJA 2002; 176 (9): 415-418
Anonymous at 6:07 AM
Monday, May 15, 2006
construction process

hi everyone. just tried to synthesize some of the information that was presented last time around into one long process chain. hopefully it makes sense.
next information/graphic will be on a comparision between an RN's and architect's perspective on the most important/frequent issues for ED planning.
s.
*edit*
here is a link to a pdf of the graphic - easier to read with clearer text.
sharon at 10:02 PM
Prediction & anticipation?
Excerpt from the talk by James Adams, M.D., 2002 about 'America's Hospitals: In Danger or Bouncing Back?'
James Adams is Professor and Chief, Emergency Medicine, Northwestern University/Northwestern Memorial Hospital
This is an example of a line graph that charts the numbers of patients registered, treated, and admitted to Northwestern Memorial Hospital over a 2 week period. Such a record of numbers can be used to help predict the number of patients admitted through the Emergency Department (ED).
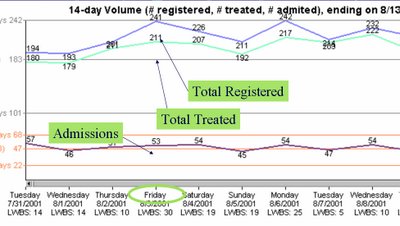
We can predict problems tomorrow by projecting, 24 hours in advance:
* Anticipated ED volume.
* Surgical volume.
* Anticipated discharges.
* Transfers/direct admissions.
* Current hospital volume.
Why would we want to predict problems?
* If we can predict problems that will occur tomorrow, we can respond today.
* If we fail to adequately respond, at least we can:
o Know that we are optimally managing the system.
o Figure out ways to manage better.
o Know that there is simply no capacity!
Once we predict a problem, then what?
* Notify medical staff.
o What do they need?
* Notify managers and key leaders.
o What do they need?
* Prioritize work to be done:
o Labs, radiology.
o Placement, rides home.
How can we begin this process?
* The hospital system must work together as a whole.
* The demands of the ED, including bottlenecks, must be monitored.
o 5 level, ESI Triage.
o Real time process controls.
+ Information tools.
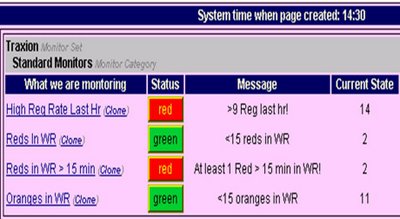
If we monitor the hospital 24 hours in advance of problems, we also must monitor the ED on a real-time basis in order to identify unanticipated problems, bottlenecks, and surges.
This is a picture of a screen showing a real-time monitoring system report. It shows what is being monitored, the status of that situation, and brief messages regarding that situation.
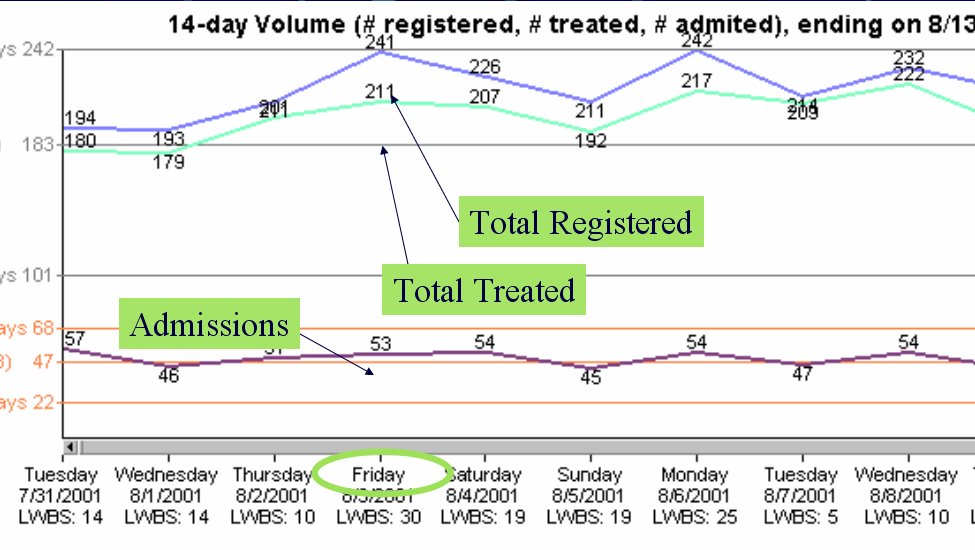
This is an example of a line graph that charts the numbers of patients registered, treated, and admitted to Northwestern Memorial Hospital over a 2 week period. Such a record of numbers can be used to help predict the number of patients admitted through the Emergency Department (ED).
We can predict problems tomorrow by projecting, 24 hours in advance:
* Anticipated ED volume.
* Surgical volume.
* Anticipated discharges.
* Transfers/direct admissions.
* Current hospital volume.
Why would we want to predict problems?
* If we can predict problems that will occur tomorrow, we can respond today.
* If we fail to adequately respond, at least we can:
o Know that we are optimally managing the system.
o Figure out ways to manage better.
o Know that there is simply no capacity!
Once we predict a problem, then what?
* Notify medical staff.
o What do they need?
* Notify managers and key leaders.
o What do they need?
* Prioritize work to be done:
o Labs, radiology.
o Placement, rides home.
How can we begin this process?
* The hospital system must work together as a whole.
* The demands of the ED, including bottlenecks, must be monitored.
o 5 level, ESI Triage.
o Real time process controls.
+ Information tools.
If we monitor the hospital 24 hours in advance of problems, we also must monitor the ED on a real-time basis in order to identify unanticipated problems, bottlenecks, and surges.
This is a picture of a screen showing a real-time monitoring system report. It shows what is being monitored, the status of that situation, and brief messages regarding that situation.

cati at 1:25 PM
Emergency Department Overcrowding
Excerpt of "Emergency Department Overcrowding and Ambulance Diversion." by Robin Weinick, Ph.D., 2002.
Robin Weinick, PhD., is Director, Intramural Research, Center for Primary Care Research, Agency for Healthcare Research and Quality
What is ED Overcrowding?
* Need for emergency services outstrips available resources in the ED.
* More patients than staffed ED beds, plus long wait times.
* Patients typically treated and monitored in hallways.
* Constrains ability to triage patients.
Measuring Overcrowding
* No established way to measure.
o AHRQ is developing a set of measures.
* Time from arrival to physician contact.
* Number of patients being boarded.
* Boarding time.
* Time on ambulance diversion.
Ambulance Diversion
* Closed to ambulance traffic.
o A symptom, not the primary problem.
* Results in:
o Increased ambulance cycle/response time.
o More first-time patients.
o Forced override.
* Measured by the number of hours on divert.
What is ED Overcrowding?
* Need for emergency services outstrips available resources in the ED.
* More patients than staffed ED beds, plus long wait times.
* Patients typically treated and monitored in hallways.
* Constrains ability to triage patients.
Measuring Overcrowding
* No established way to measure.
o AHRQ is developing a set of measures.
* Time from arrival to physician contact.
* Number of patients being boarded.
* Boarding time.
* Time on ambulance diversion.
Ambulance Diversion
* Closed to ambulance traffic.
o A symptom, not the primary problem.
* Results in:
o Increased ambulance cycle/response time.
o More first-time patients.
o Forced override.
* Measured by the number of hours on divert.
Percent of Hospitals 'At' or 'Over' Capacity
This bar graph provides percentages of four different types of hospitals that reported being "at" or "over" capacity in 2002. The types of hospitals and the percentage reporting capacity issues are as follows: 79% of all urban hospitals; 45% of rural hospitals; 81% of teaching hospitals; and 56% of non-teaching hospitals. Nationally, 62% of all hospitals reported capacity issues.
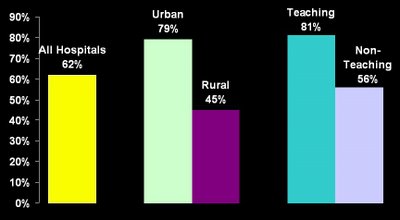
Source: The Lewin Group Analysis of AHA ED and Hospital Capacity Survey, 2002
The percentages of hospitals in the following groupings reported being 'at' or 'over' capacity: 34% of hospitals with less than 100 beds reported problems; 77% of hospitals with 100-299 beds were "at" or "over" capacity; 91% of hospitals with 300-499 beds reported capacity issues; and 90% of hospitals with more than 500 beds had capacity problems. In terms of trauma levels, 87% of level I hospitals reported capacity issues and 79% of level II reported capacity problems.
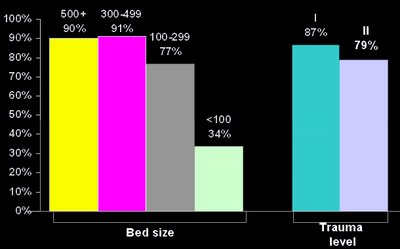
Source: The Lewin Group Analysis of AHA ED and Hospital Capacity Survey, 2002.
This bar graph provides percentages of four different types of hospitals that reported being "at" or "over" capacity in 2002. The types of hospitals and the percentage reporting capacity issues are as follows: 79% of all urban hospitals; 45% of rural hospitals; 81% of teaching hospitals; and 56% of non-teaching hospitals. Nationally, 62% of all hospitals reported capacity issues.

Source: The Lewin Group Analysis of AHA ED and Hospital Capacity Survey, 2002
The percentages of hospitals in the following groupings reported being 'at' or 'over' capacity: 34% of hospitals with less than 100 beds reported problems; 77% of hospitals with 100-299 beds were "at" or "over" capacity; 91% of hospitals with 300-499 beds reported capacity issues; and 90% of hospitals with more than 500 beds had capacity problems. In terms of trauma levels, 87% of level I hospitals reported capacity issues and 79% of level II reported capacity problems.

Source: The Lewin Group Analysis of AHA ED and Hospital Capacity Survey, 2002.
How Many ED Visits? 1992-2000
This bar graph tells how many visits were made nationwide to Emergency Departments. The number of visits by year are: 1992: 91 million; 1993: 90 million; 1994; 93 million; 1996: 90 million; 1998: 100 million; 2000: 108 million. The number of ED visits nationally has increased by 20% between 1996 and 2000.
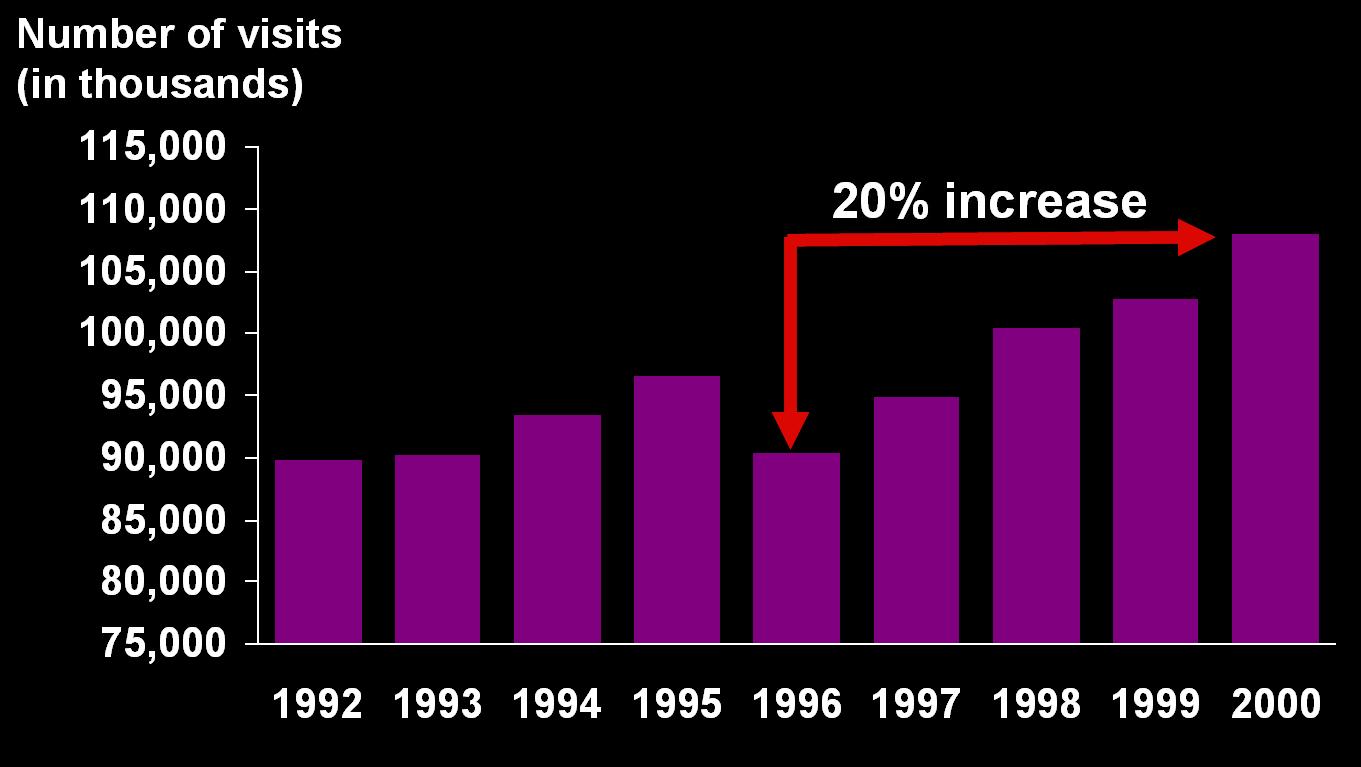
Source: National Center for Health Statistics, National Hospital Ambulatory Medical Care Survey, 1992-2000.
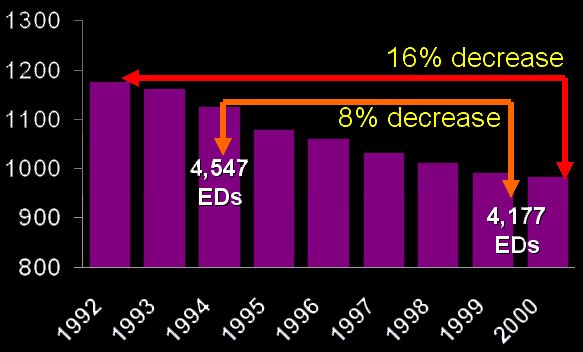
How Many Hospital Beds? 1992-2000
This graph highlights the reduced supply of both hospital beds and Emergency Departments across the nation. From 1992-2000 there was an overall 16% decrease in the number of hospital beds and an 8% decrease in the number of Emergency Departments.
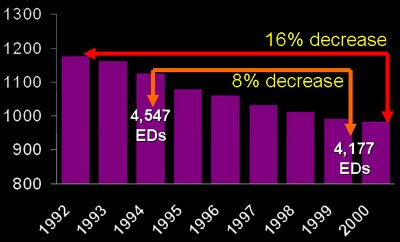
Source: American Hospital Association, Hospital Statistics.
This graph highlights the reduced supply of both hospital beds and Emergency Departments across the nation. From 1992-2000 there was an overall 16% decrease in the number of hospital beds and an 8% decrease in the number of Emergency Departments.
Source: American Hospital Association, Hospital Statistics.
How are Hospitals Staffed?
This graph shows the total number of new Registered Nurse graduates between 1995 and 2000. Highlighted on this slide is the fact that between 1995 and 2000, the number of new RNs has decreased by 26%.
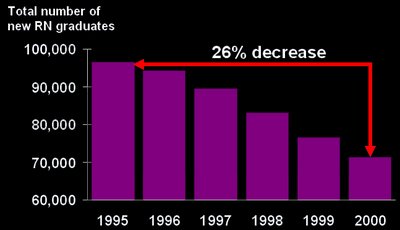
Source: Health Resources and Services Administration, "Projected Supply, Demand, and Shortages of Registered Nurses: 2000-2020."
Source: American Hospital Association, Hospital Statistics.
This graph shows the total number of new Registered Nurse graduates between 1995 and 2000. Highlighted on this slide is the fact that between 1995 and 2000, the number of new RNs has decreased by 26%.

Source: Health Resources and Services Administration, "Projected Supply, Demand, and Shortages of Registered Nurses: 2000-2020."
Source: American Hospital Association, Hospital Statistics.
cati at 12:49 PM
Growing Demand for Emergency Room Visits AndThe Addition of New Hospitals
On November 19, 2002, Stuart Altman, Ph.D., made a presentation in a Web-assisted teleconference at Event 1, which was entitled "The Big Picture: Hospitals in a Volatile Healthcare Environment." He mentionned the Growing Demand for Emergency Room Visitsand the Addition of New Hospitals.
Stuart Altman, PhD, is Chaikin Professor of National Health Policy, The Florence Heller School of Public Health, Brandeis University
Few elements that I have kept from his talk are:
o Increased Inpatient Utilization.
o Continued Growth in Outpatient Use.
o Increased ED Use.
* Accelerating Cost of Services.
* But, Inadequate Payment Rates from:
o Medicaid.
o Uninsured.
o Medicare.
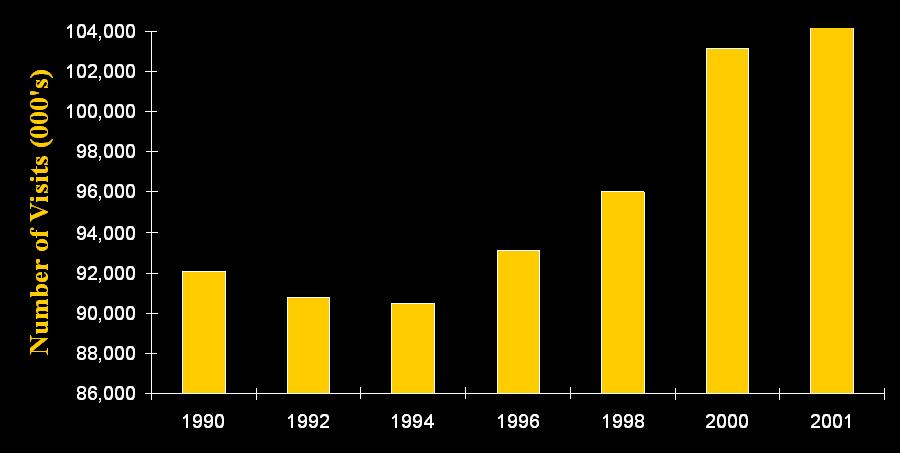
This bar graph provides national estimates of the number of Emergency Department visits by year. The numbers of visits were: 1990, 92 million; 1992, 91 million; 1994, 90 million; 1996, 93 million; 1998, 96 million; 2000, 103 million; and in 2001, 110 million.
The projections prepared by the Advisory Board on how many more hospitals will be needed by the year 2011 based upon different sets of assumptions: A conservative estimate puts the additional number of hospitals needed at 1,023, a moderate estimate at 2,491 and an aggressive estimate at 4,914.

cati at 12:35 PM
Individual Hospital Statistics for Massachusetts
Individual Hospital Statistics for Massachusetts Staffed Beds/Gross PatientRevenue, from the AHD

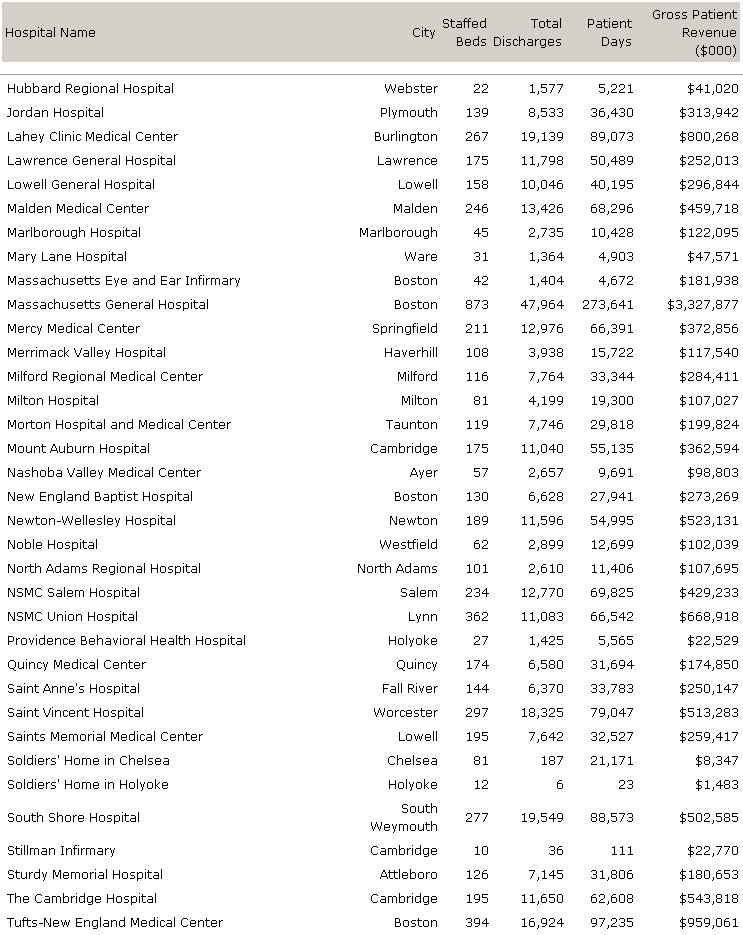

A total of 13,850 staffed beds
cati at 12:23 PM
US national hospital data
Statistics for non-federal, short-term, acute care hospitals from the American Hospital Directory.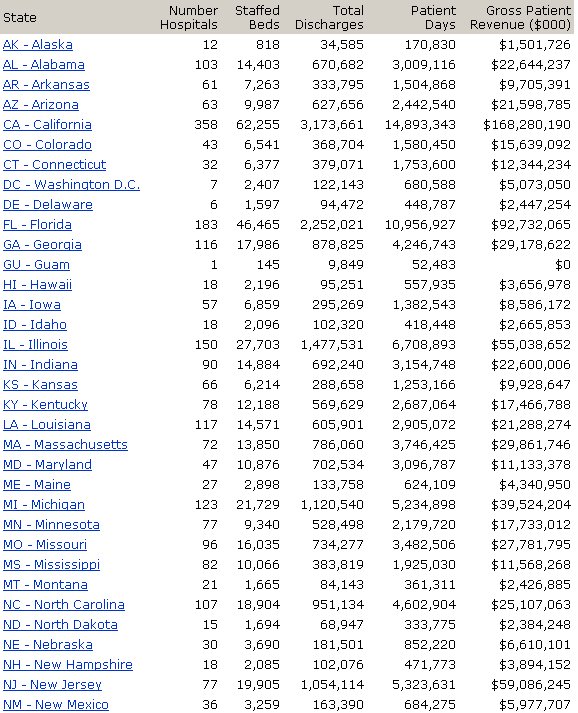

A total of 660,558 staffed beds for 4,019 hospitals
cati at 12:14 PM
Coordinating communication among and enhancing the efficiency of providers of EMS including ambulance services in the MA
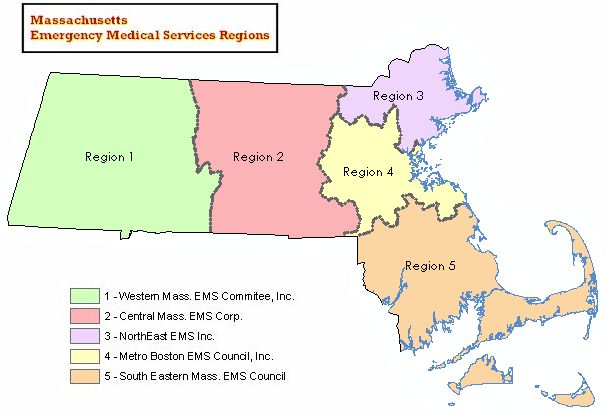
Emergency Medical Services (EMS) Regions are designated by the Massachusetts Department of Public Health Office of Emergency Medical Services (OEMS). Grouped by municipality, each EMS region is administered by a regional office dedicated to promoting patient care by coordinating communication among and enhancing the efficiency of providers of EMS including ambulance services, first responders and hospital emergency departments. Educational and training programs are also offered
cati at 11:04 AM
Saturday, May 13, 2006
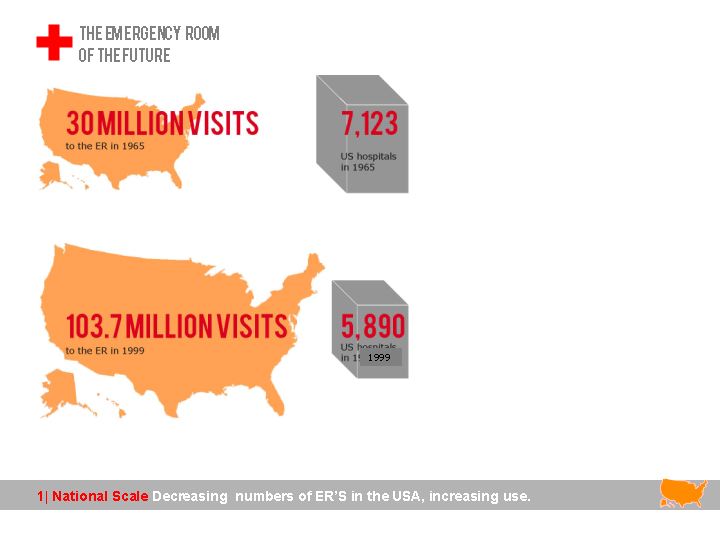
Presentation for Tuesday: progress update
I have been laying out the powepoint for Tuesday, here are JPEGS of the slides.










Anonymous at 9:00 PM