Friday, April 14, 2006
Triage
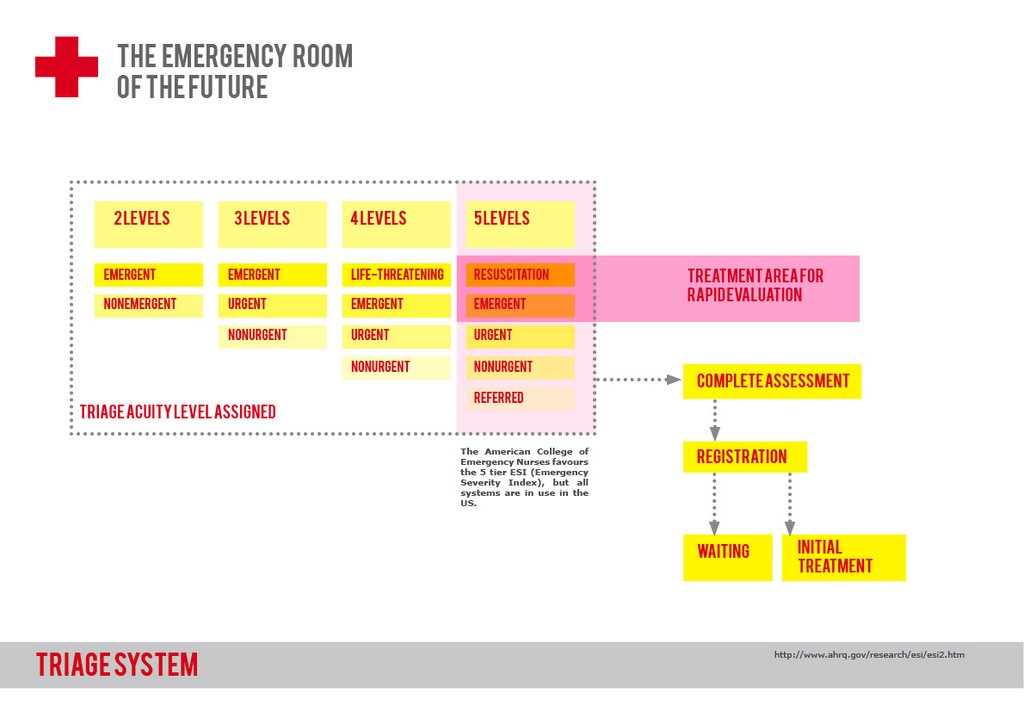
Anonymous at 5:58 AM
Thursday, April 13, 2006
Typologies and Spatial Analysis
In an attempt to understand how actual Emergency Rooms function we have consulted and visited with medical professionals immersed in the actual ER environment. While, admittedly, their design knowledge and opinions may be lacking, their understanding of the practical, actual, and utilitarian experiences can help us better understand the space. As designers it then becomes our task to decipher the design qualities that contribute to certain preferences.Interpretations of ER Descriptions
The following three hospitals are interpretations of spaces either described by medical workers or by site visits.
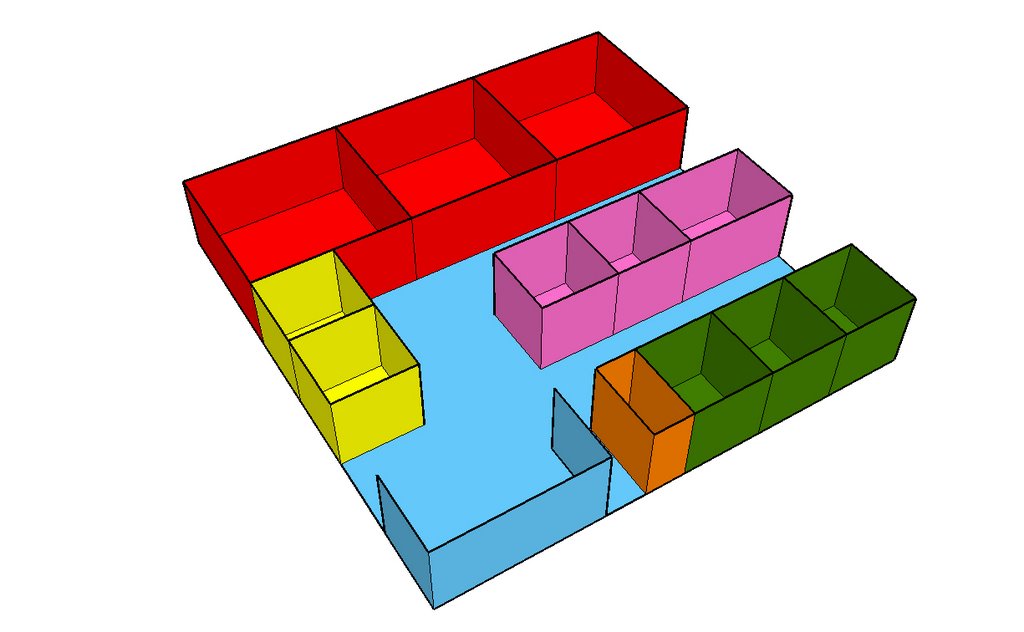
 University Hospital - New Jersey
University Hospital - New Jersey This first example is of University Hospital in New Jersey as described in a conversation with Ershad Elahi, a third year medical student at the New Jersey Medical School. The unique thing about this layout is that patients are immediately separated into two different categories: trauma and medical. This allows for a specialization of care that helps make the process smoother. While such a system does require essentially two distinct and complete staff, a well thought layout can utilize shared resources such as supplies and OR rooms.
 Rochester Emergency Facilities
Rochester Emergency FacilitiesThis second example, also described during a conversation with Ershad Elahi, is a layout of the Rochester Emergency Facilities. Unlike the linear example above, this plan is set up radially. The patient and OR rooms are placed at the perimeter of the plan to provide visual and circulatory access to the core of the building which is staffed with nurses and doctors. The supplies are central to the plan giving equal access to all those who might need it. As organized according to the conversation, it seems that this layout limits both expansion and access. However it does provide a fairly successful circulation scheme.
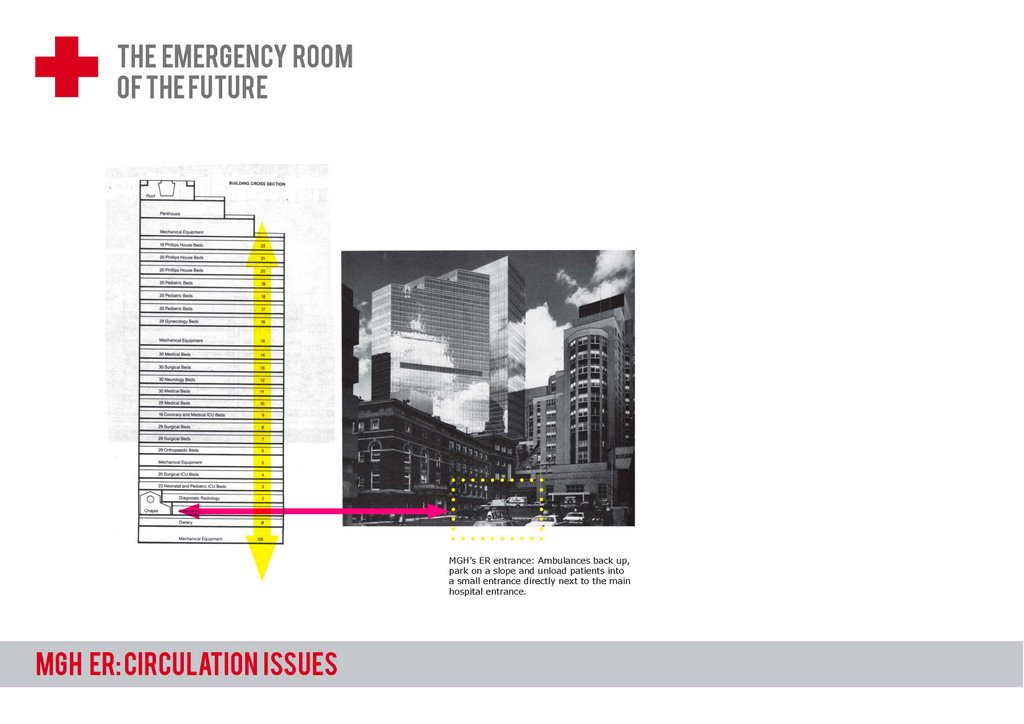
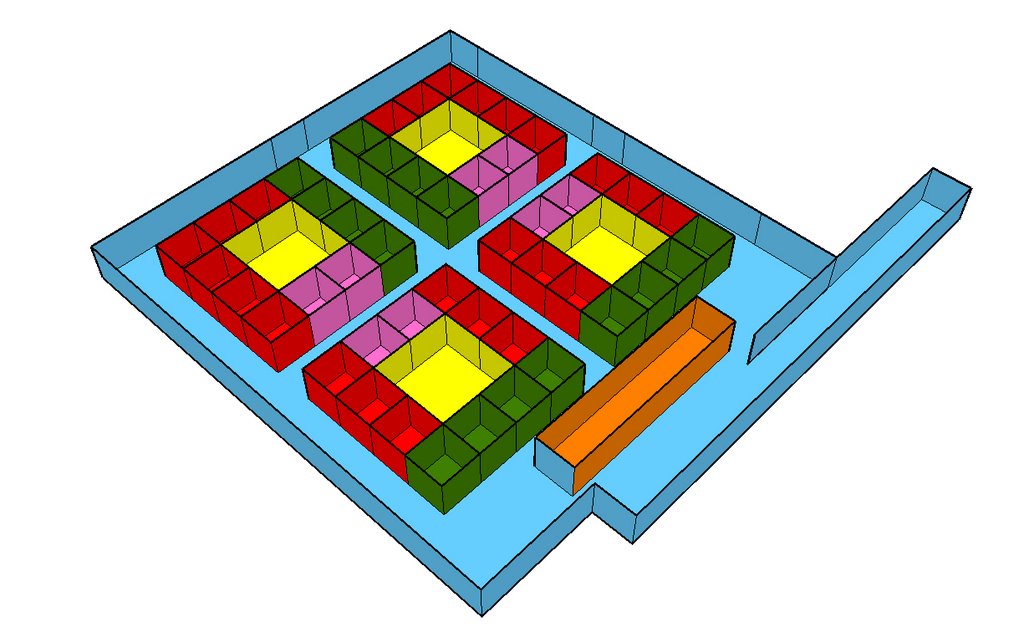 MGH: An Abstract Impression
MGH: An Abstract ImpressionOur visit to the emergency room at MGH was quick and disorienting, although quite educational. The space and layout was extremely difficult to understand in a short and furious tour through the facility. However, this layout explains the general impression of the space. This layout may be described as nodal, where particular functions and specialties pop up in concentrated cores of activity. Each core then becomes able to handle it's own nursing staff, doctors, technological support, specialty rooms, patient rooms and supplies. While as confusing to navigate as a McMansion suburban neighborhood, it is actually a very flexible system that allows for expansion in the long run.
Generic Hospital Layouts
Many of our sources often point generic plans to stress a point about trends in design and layout. The following three examples are just a sampling of the information that is out there on spatial analysis.
 Generic Layout 1
Generic Layout 1This layout, taken from Design Planning for Ambulatory Care Facilities shows a typical one way circulation system. The plan has a strong orientation that explains the process through the ER. Successful aspects of this design include access to the supplies and the nurses station from the important medical rooms (such as OR or Radiology). Some of the drawbacks of such a plan include the privacy issues associated with a large patient recovery room and the relative distance from things the further you make your way through the circulation diagram.
 Generic Layout 2
Generic Layout 2This plan, taken from Hospital Emergency Facilities uses some fairly typical layout strategies. First of all, it separates the patient rooms from the important activities in the hospital. In the buffer between these two you will find both supplies and the nurses/medical staff facilities. This buffer zone then allows for access of the staff and supplies both to the high resource side rooms and the patient rooms. Although the zones are clearly delineated, the segregation may be detrimental in the long run when it comes time for expansion. It might be nice to see this approach in a more "branched" layout.
 Generic Layout 3
Generic Layout 3Also from Hospital Emergency Facilities this layout separates more clearly the more important rooms of the ER from the rest of the program. This can be beneficial down the road because the integration of new technological or machine heavy equipment can be a hassle to integrate fully into a fixed plan. The peripheral quality of the more significant program will facilitate expansion and changes in medicine and technology. This is also a good example of clearly delineated entrances for walk-ins and ambulatory access. Another interesting thing about this layout is the mixing of nurses stations and supply closets. It seems that this then allows for greater access to more patients when such a system is not afforded (as in a radially scheme)
Typological Layouts
We have also been investigating generic strengths and weaknesses of hospital and ER typologies. The following three examples begin to stress some of the more pressing issues at hand when planning hospitals.
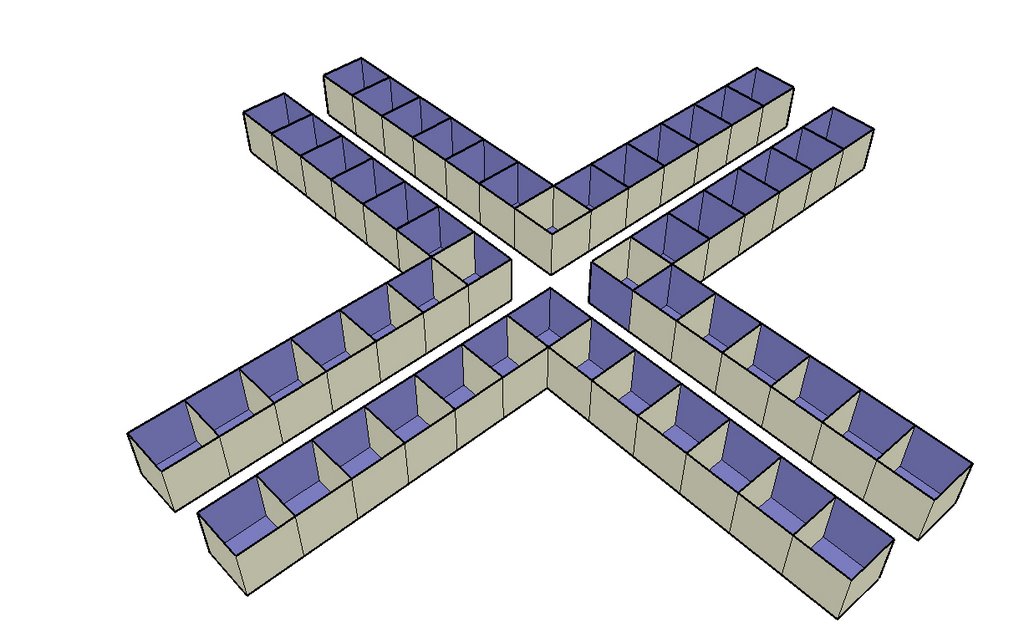 The Cross
The CrossA crucifix layout is strong in it's ability to distribute double-loaded program in the shortest walking distance. However it become very important to think about where shared resource are located. For instance, if the arms of the cross become specialized then it's difficult to determine the appropriate location for supplies, nurses stations, staff resting rooms, and ORs. However expansion, if there is room, is easier in an "appendage" plan because it takes less room to add on.
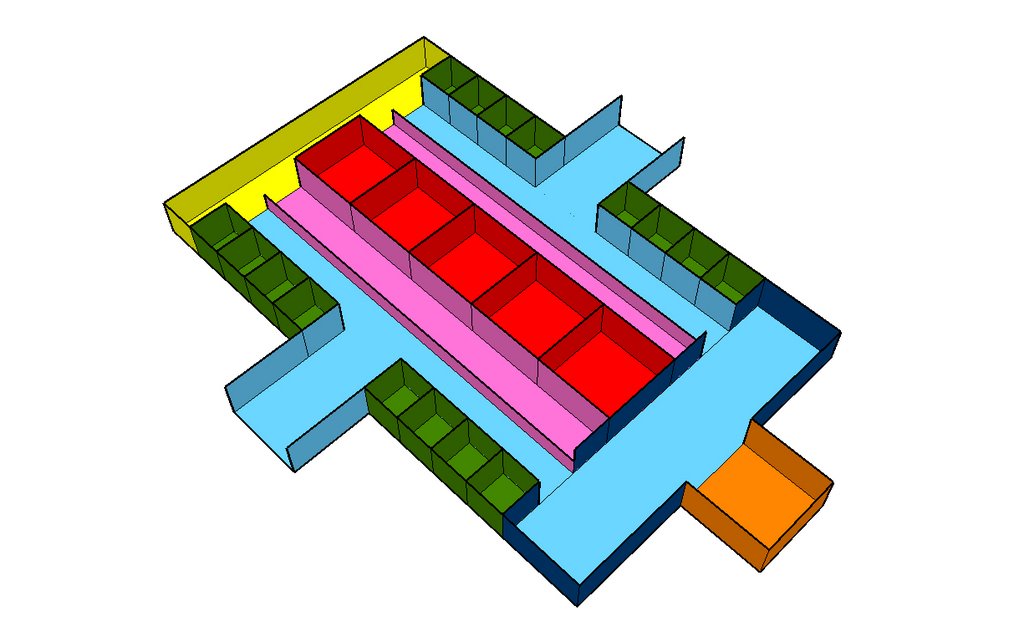
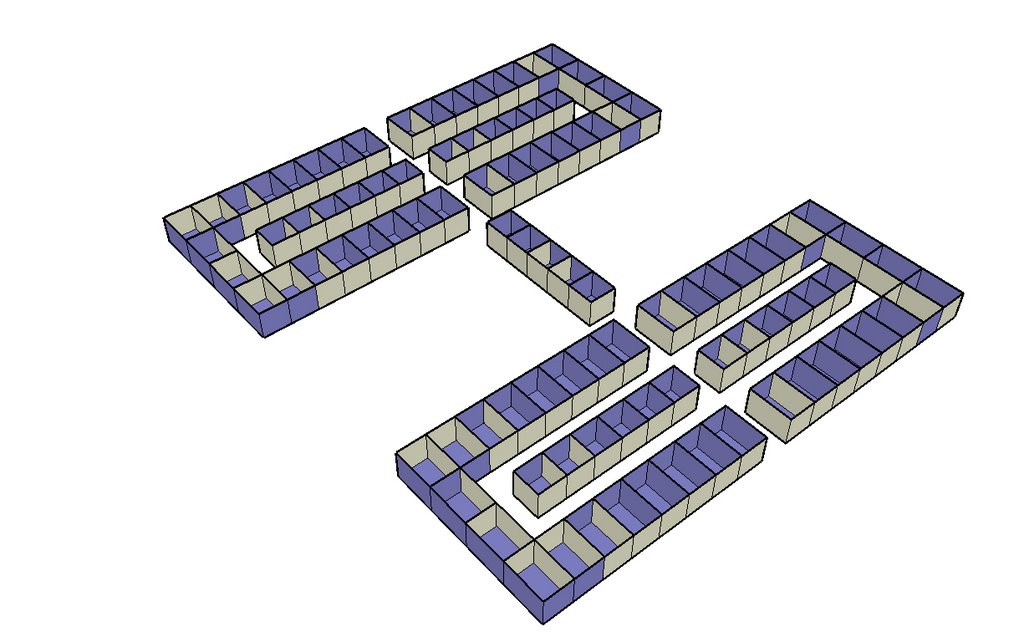 The Racetrack
The RacetrackThis plan is a good way to keep diverse programs in close proximity to each other. However, a drawback is that circulation quickly becomes long and disorienting. The strength in executing a plan like this would be to use the middle spaces as a transition space between one side of the hall and the other. This plan also allows for a certain degree of specialization.
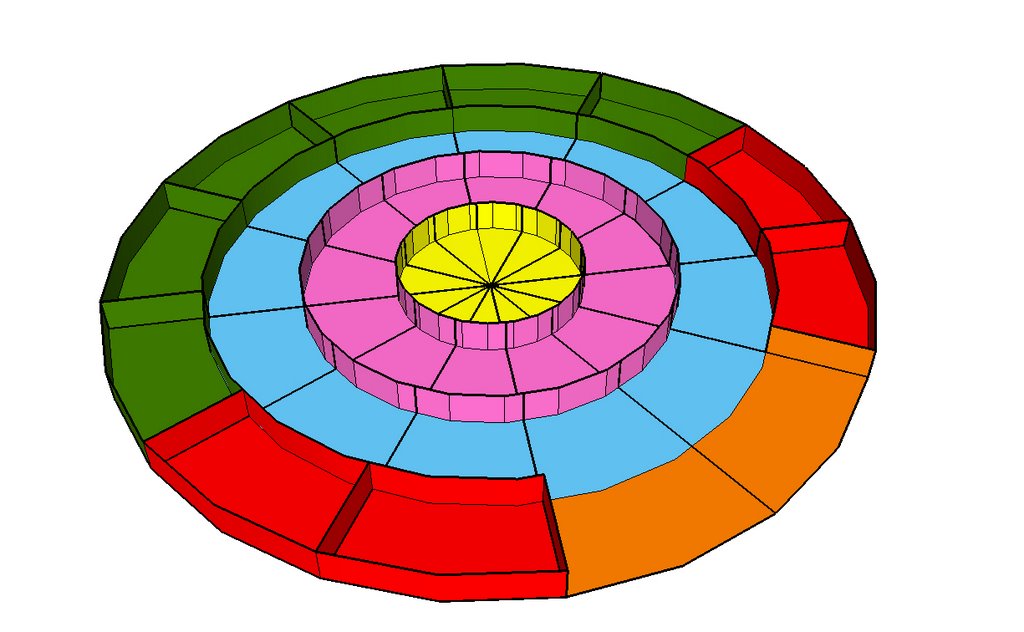
 Radial
RadialThe radial plan, as seen earlier in an interview interpretation, is straightforward in it's approach to organizing circulation and programmatic overlap. The biggest downside of such a plan is that it is limited in capacity. To add another ring increases the built area exponentially and increase circulation difficulties. Ideally a radial plan would have supplies and medical staff located centrally so as to be easily distributed to the circumference. It is also interesting to note the varying types of private and public circulation, from the external car down to private medical staff.
Anonymous at 11:59 PM
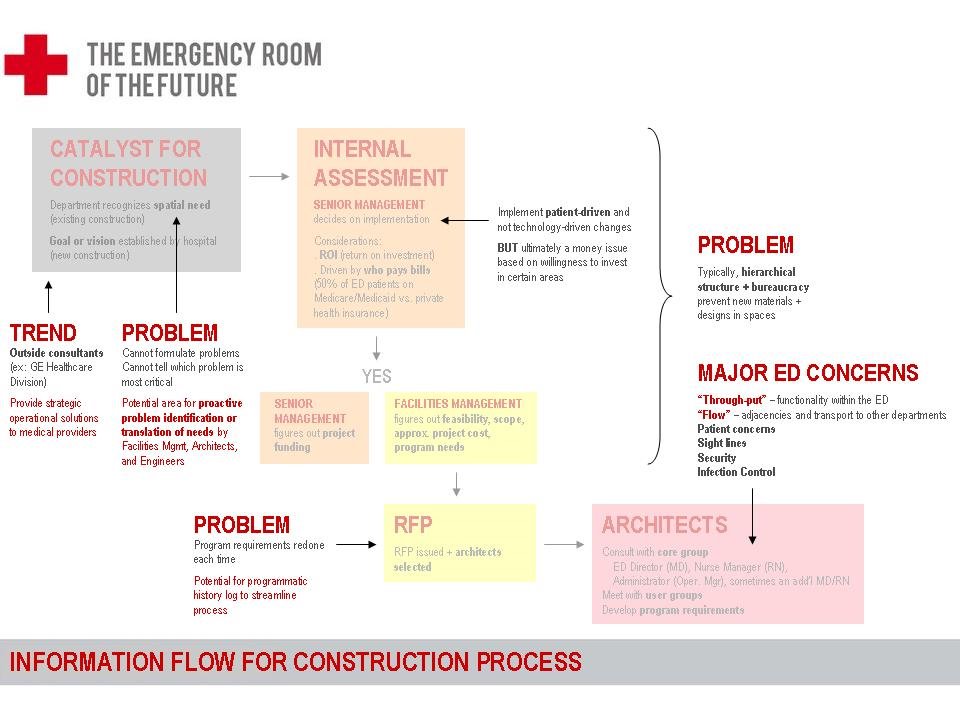
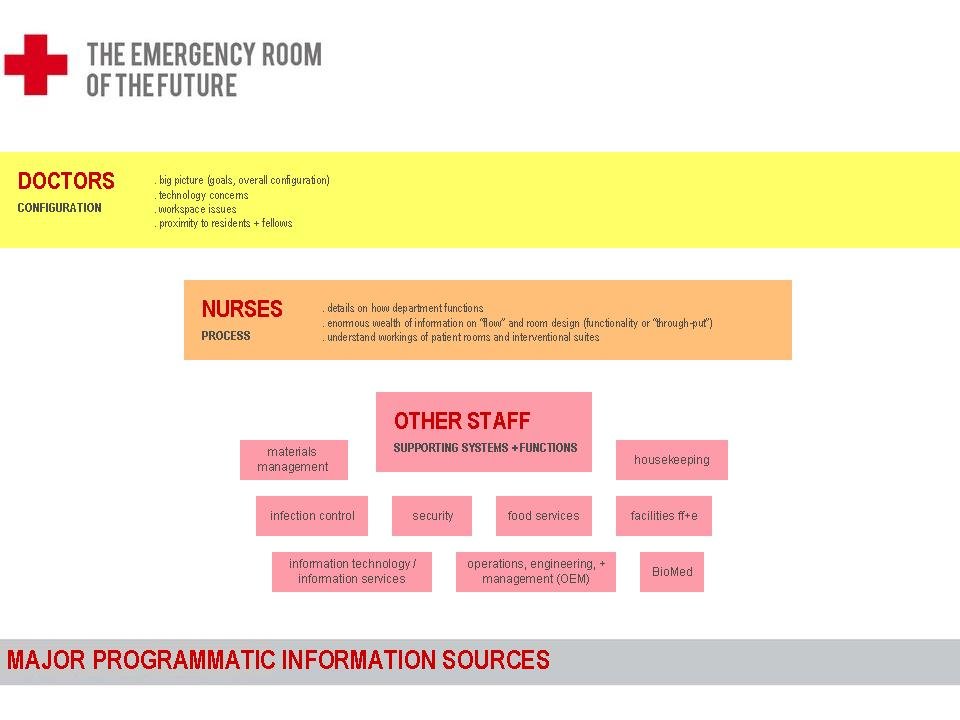
information for construction process
here are some blocky diagrams trying to sort the information utilized in the construction process for an ED: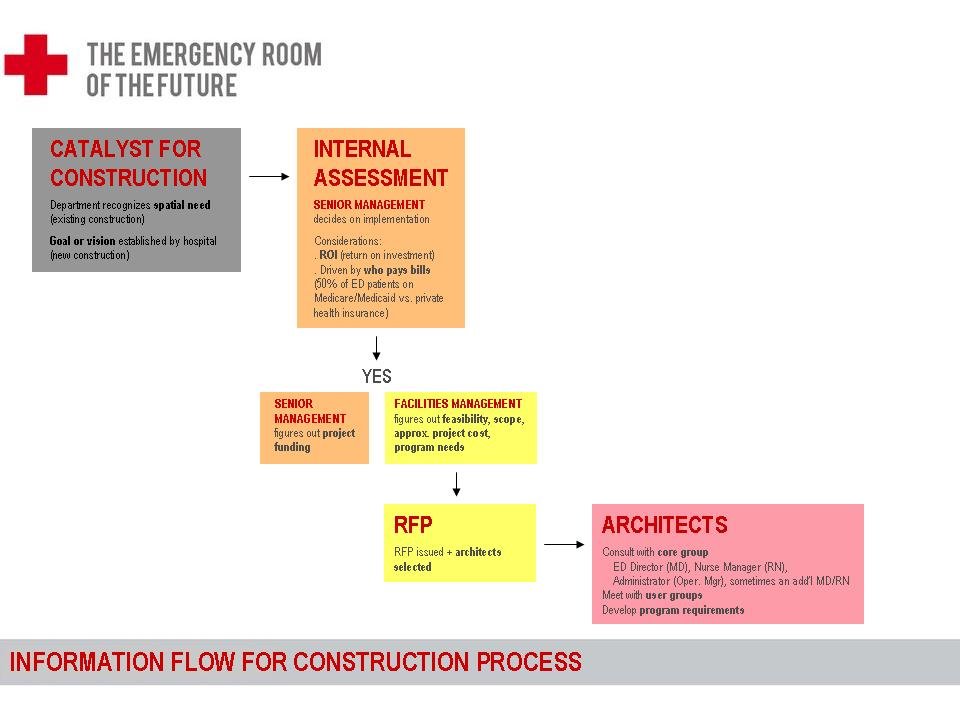
sharon at 9:27 PM
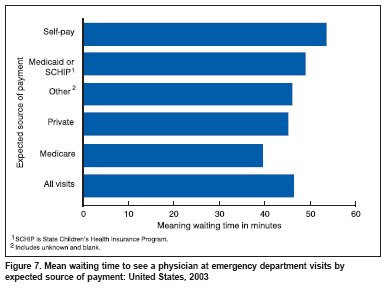
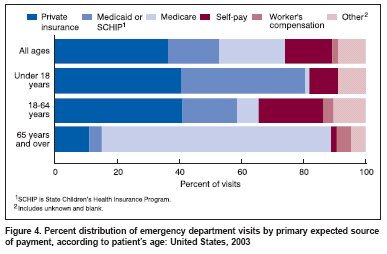
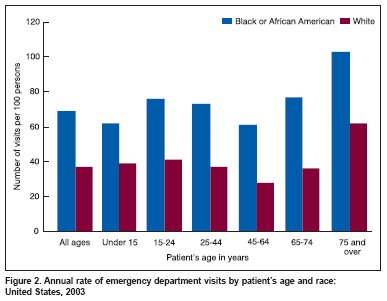
Emergency Department Visit Data



{kind=link}
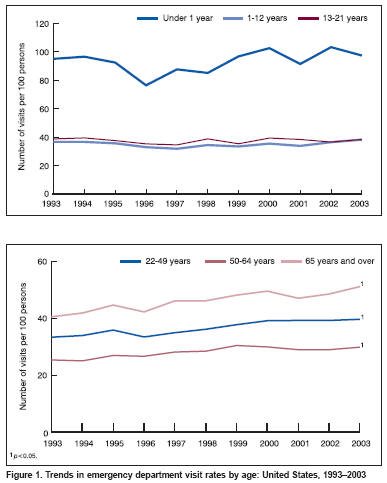
The following figures were excerpted from McCaig LF, Burt CW. National Hospital Ambulatory Medical Care Survey: 2003 emergency department summary. Advance data from vital and health statistics; no. 358. Hyattsville, MD: National Center for Health Statistics. 2005.
cati at 3:39 PM
MGH ER analysis

Anonymous at 12:06 PM
Wednesday, April 12, 2006
American ER Today
Here is a preliminary attempt at devising a way of presenting all the stats.
Has anyone collected information on TRIAGE, or any other ER processes as I would like to do some systems diagrams for Friday.
I have a couple of contacts at the medical school, who are happy to answer questions from the medical standpoint/recommend books from HMS library. Any burning questions that I can put to them?
Anonymous at 12:28 PM
Tuesday, April 11, 2006
Principal Design Issues in the ER

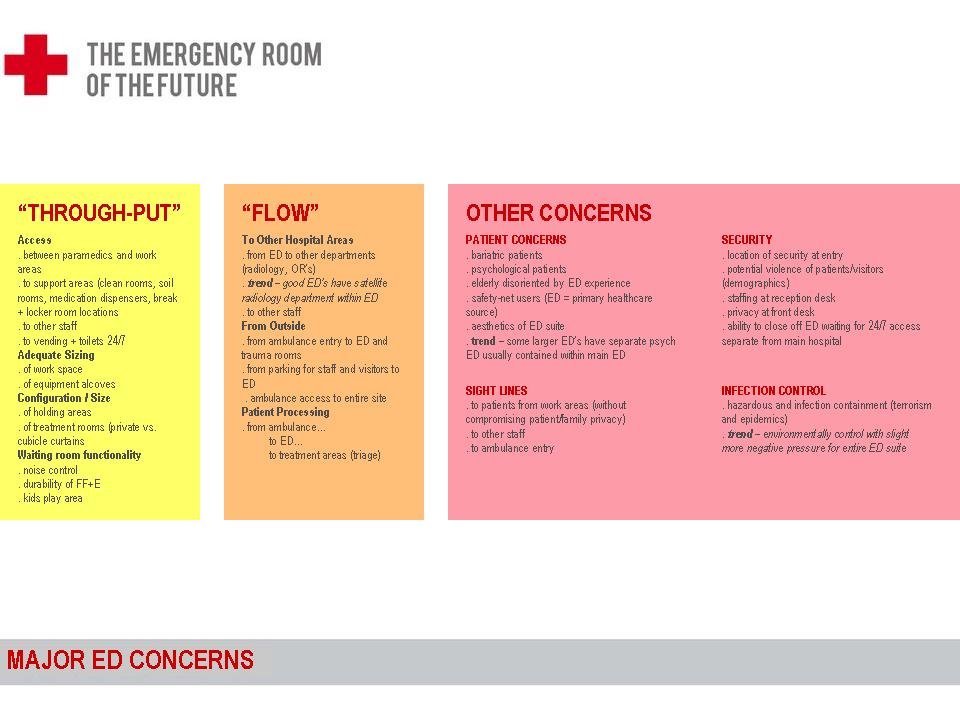
PRINICIPAL DESIGN ISSUES
- Helicopter access
- Triage
- The waiting area
- Treatment spaces
o Triage area
o Trauma room (s)
o Cardiac resuscitation room (s)
o Urgent exam room/treatment room (s)
o Non-urgent exam room/treatment room (s)
o Geriatric treatment room (s)
o Suture/minor treatment room (s)
o Quiet room (s)
o Secure isolation room for psychiatric emergencies (s)
o Paediatric treatment/examination room (s)
o OB-GYN room (s)
o Eye examination room (s)
o Cast/ortho room
o Decontamination room (s)
o Observation room (s)
o Chest pain observation room (s)
o Fast-track room for primary care (s)
o Emergency dental treatment room (s)
- Staff and support spaces
- Accommodation of data and diagnostic technologies
- Flexible design for flexible response
- Specialty emergency treatment areas
- Security
- Convenient parking
- Prominent signage and entryways
OTHER GENERAL ISSUES TO CONSIDER IN ER DESIGN
- Layout: satellite vs. ballroom vs. corridor vs. pods etc.
- Are the patients observing what is going on more than the staff is able to?
- How to prevent patients being ‘forgotten about’
- How to improve the experience for the patient
- Enormous waiting times: 5 hours
- Overcrowding
- 30% of the population are without medical insurance
- ER as primary care facility (esp. for those without insurance)
- ED running at a deficit in most cases: how can profitability be improved?
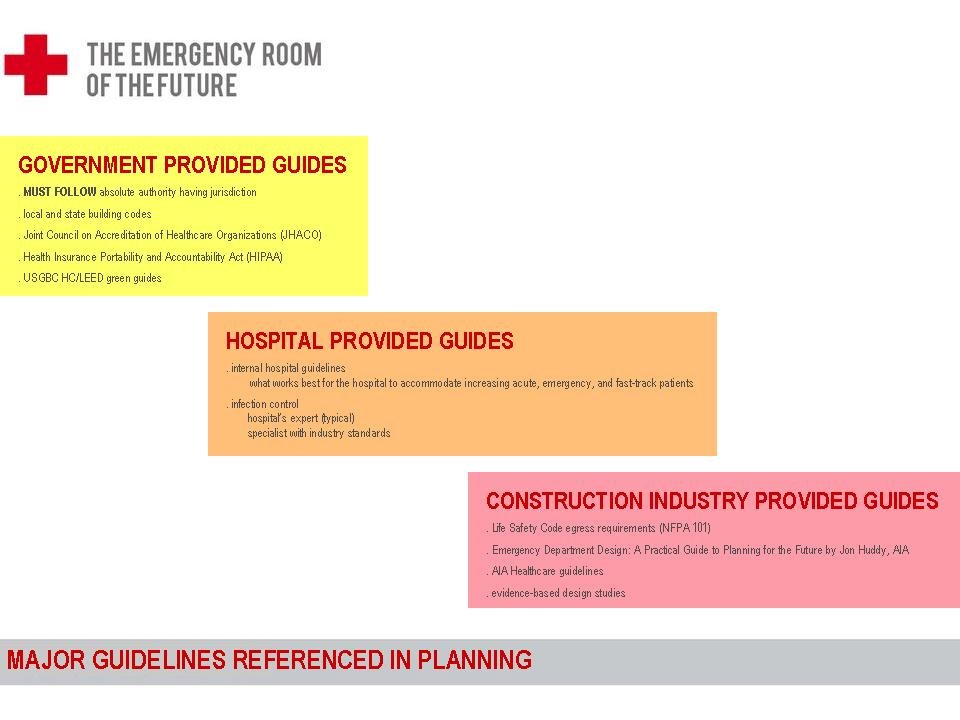
BIBLIOGRAPHY
Chapter on Boston City Hospital
Vogel, M. J., The Invention of the Modern Hospital, University of Chicago Press, 1980
Miller, R. L. and Swensson, E. S.. Hospital and Healthcare Facility Design, W.W. Norton and Company, 2002. Chapter 5
Guidelines for Design and Construction of Hospital Facilities, AIA Press, 1997
Zimring, C. A Guide to Conducting Healthcare Facility Visits, The Centre for Healthcare Design, 1994
Lennon, J. A Workshop for Designing the ER of the Future Journal of Healthcare Design, Volume XIII 1996 p. 139
Anonymous at 1:11 PM
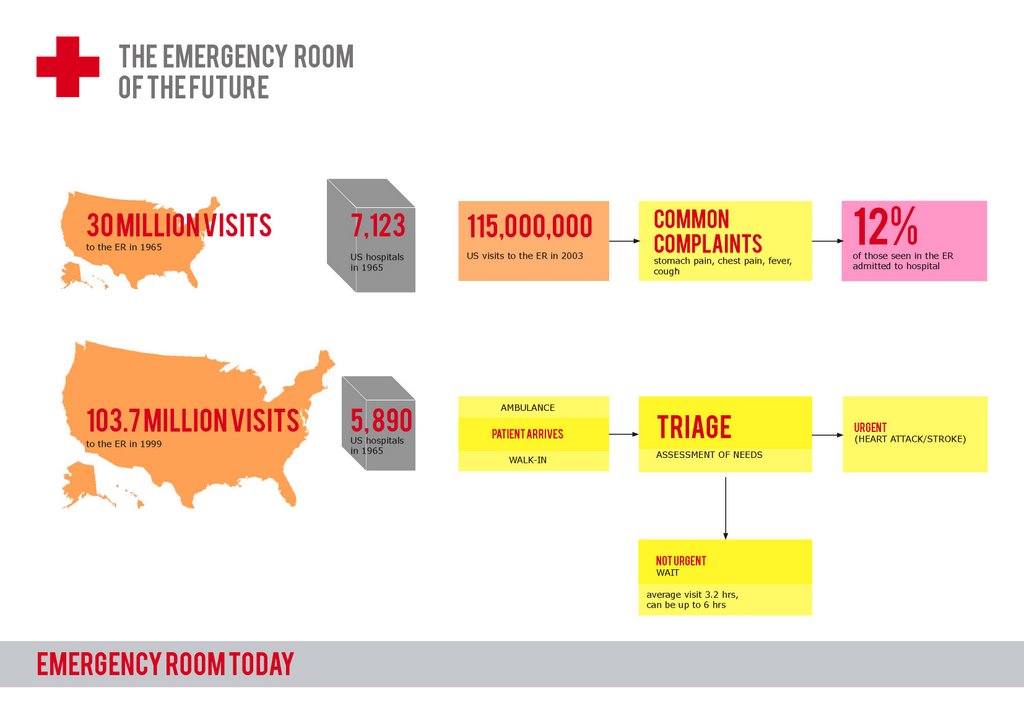
The ER today
In 1965, there were 30 million visits to the ER; in 1999 there were 103.7 million visits to the ER.US hospitals in the same period dropped from 7,123 to 5,890.
According to the American College of Emergency Physicians, Americans made more than 115 million visits to hospital emergency rooms in 2003. Some of the most common complaints were stomach pain, chest pain, fever and cough. About 12 percent of those seen in the emergency room are admitted to the hospital.
The National Hospital Ambulatory Medical Care Survey found in 2002, the average duration of a visit to the emergency room was 3.2 hours. However, the actual range of waiting time varied, with some patients waiting as long as 6 hours.
More...
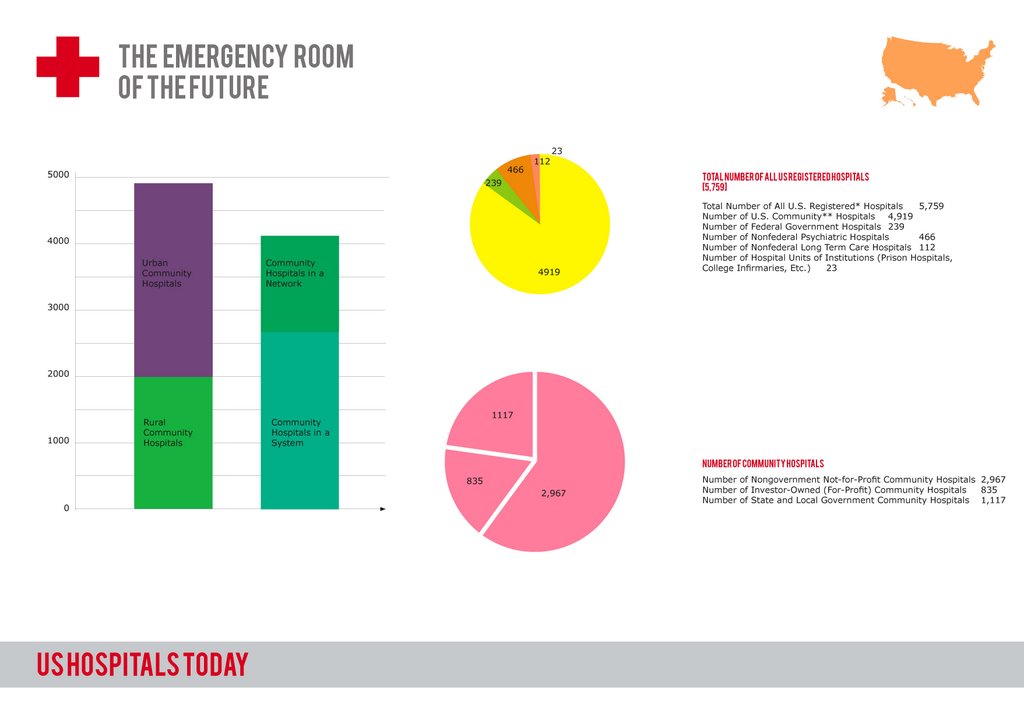
FACTS ON US HOSPITALS FROM AHA HOSPITAL STATISTICS
The American Hospital Association conducts an annual survey of hospitals in the United States. The data below is from the 2004 annual survey.
Total Number of All U.S. Registered* Hospitals 5,759
Number of U.S. Community** Hospitals 4,919
Number of Nongovernment Not-for-Profit Community Hospitals 2,967
Number of Investor-Owned (For-Profit) Community Hospitals 835
Number of State and Local Government Community Hospitals 1,117
Number of Federal Government Hospitals 239
Number of Nonfederal Psychiatric Hospitals 466
Number of Nonfederal Long Term Care Hospitals 112
Number of Hospital Units of Institutions (Prison Hospitals,
College Infirmaries, Etc.) 23
Total Staffed Beds in All U.S. Registered* Hospitals 955,768
Staffed Beds in Community** Hospitals 808,127
Total Admissions in All U.S. Registered* Hospitals 36,941,951
Admissions in Community** Hospitals 35,086,061
Total Expenses for All U.S. Registered* Hospitals $533,853,359,000
Expenses for Community** Hospitals $481,246,587,000
Number of Rural Community** Hospitals 2,003
Number of Urban Community** Hospitals 2,916
Number of Community Hospitals in a System*** 2,669
Number of Community Hospitals in a Network**** 1,464
*Registered hospitals are those hospitals that meet AHA's criteria for registration as a hospital facility. Registered hospitals include AHA member hospitals as well as nonmember hospitals. For a complete listing of the criteria used for registration, please see Registration Requirements for Hospitals .
**Community hospitals are defined as all nonfederal, short-term general, and other special hospitals. Other special hospitals include obstetrics and gynecology; eye, ear, nose, and throat; rehabilitation; orthopedic; and other individually described specialty services. Community hospitals include academic medical centers or other teaching hospitals if they are nonfederal short-term hospitals. Excluded are hospitals not accessible by the general public, such as prison hospitals or college infirmaries.
***System is defined by AHA as either a multihospital or a diversified single hospital system. A multihospital system is two or more hospitals owned, leased, sponsored, or contract managed by a central organization. Single, freestanding hospitals may be categorized as a system by bringing into membership three or more, and at least 25 percent, of their owned or leased non-hospital preacute or postacute health care organizations. System affiliation does not preclude network participation.
**** Network is a group of hospitals, physicians, other providers, insurers and/or community agencies that work together to coordinate and deliver a broad spectrum of services to their community. Network participation does not preclude system affiliation.
Anonymous at 1:01 PM
Visit to Massachusetts General Hospital ER

MRI Image from General Electric Healthcare
Interview with Dr. Gonzalez, Chief of Neuroradiology at the Massachusetts General Hospital and Associate Professor of Radiology at Harvard Medical School.
QUESTIONS
1. How do patients transfer to specialists in two hypothetical situations?
a. Clear-cut situation such as a broken limb
b. Less obvious situation: how many steps before radiological imaging is called for?
2. What is the head radiologist's dream ER and how would it function?
3. How does the ER interface with other departments within the hospital (such as the psych dept)?
4. What are the major security issues and patient privacy issues?
5. What is the actual protocol for triage?
6. Is the head radiologist more of a clinical or administrative position at the hospital?
7. How much interaction does the radiology department have with the ER?
8. What types of comments come back from staff and patients?
9. How are patients physically transferred between departments?
10. What are the time constraints? What are the time limits to treatment options?
11. How much does the clinical staff rely on patient questionnaires vs. observation?
12. What is the protocol for repeat patients?
13. How does MGH's ER compare to ER's in other hospitals?
KEY RESPONSES
TRIAGE
MGH - patient arrive mainly by ambulance rather than as walk-ins, but the ER caters to both.
The EMT makes decision where the patient should go, and assesses the situation. After the patient arrives at the ER, the Triage nurse evaluates the patient, determining whether the problem is routine or critical.
If further investigation is necessary, the patient will undergo CT scans and/or MR studies.
A hypothetical situation illustrates the breadth of response: a patient comes in with a headache, after an accident. After triage: the patient is sent home having been evaluated and given some painkillers, or will be sent to have a CT scan which may show an aneurysm and will then have to be treated. The patient will be admitted to the appropriate part of the hospital.
ISSUES OF COMMUNICATION
There is no substitute for talking face-to-face; it is the best means of communication in the ER. This includes both doctor-to-patient and especially doctor-to-doctor communication.
Transfer of information is done face-to-face.
ISSUES OF OWNERSHIP OF THE PATIENT
The ER is the entryway to the hospital. If the patient is admitted, then - for example - neurosurgeons and other specialists will take over management of the patient from the ER. The patient will not return to the ER, but will be transferred around other parts of the hospital as necessary.
ISSUES OF LEGACY OF BUILT FORM
One of the main problems is that the ER inhabits an old building. The ER is a hybrid system, which has evolved over a century, but is becoming more streamlined. The built form however, creates issues of legacy. How do you fit new machines, new ways of treating patients etc into the existing shell, whilst continuing functional operation of services within the hospital?
CARING FOR THE PATIENT IN THE ER
The main business of the ER is vital care.
Support systems: a problem is all the extra kit following patients around: trolleys and wires with IV/machines etc that have to be maneuvered individually whilst still connected to the patient.
Scanning/Docking CT/MRI procedures now take only a few minutes (CT scan possible in just 5 minutes), but the whole process can take an hour to get the patient onto and off the scanner.
The scanning machines are in use 24/7. On average, 2 patients per hour on the CT scanner, 1 per hour on the MRI scanner. Patient has to change cart due to the magnets, all needles etc have to be changed so that there is no ferrous material in the scanning room.
Issues with CT/MRI machines– placement in building, special building materials etc.
Overflow spaces (staging areas) for scanning. Scanners constantly in use.
The ER at MGH has an ER Radiology Department within the ER which is one part of a larger radiology department.
THE DREAM ER
Easier interventions and upgrades.
Patient focus/patient-centric platform
Vertical connection to the rest of the hospital from the ER.
Communications systems: face-to-face, paging, telephone instant access is important in the ER. The ideal would be to have instant video conferencing, however, this is still not a substitute for face-to-face communication, and would only be useful if was instantaneous.
GENERAL ISSUES AT MGH'S ER
Bottlenecks and tight corners. Legacy issues in every ER.
Control rooms scanning reading room (very dark).
Issues of cross-talk– privacy screen in tight spaces such as CT control rooms.
Issues of getting lost and mobility
ER's are not 'designed', at the most, they are space planned. How quickly do they go out of date? How do you upgrade them? Should equipment rooms such as scanning facilities be placed around the edges for easy upgrading of large equipment? Are things already out of date by the time they are built and start to be in use?
Trolleys that automatically cart medical supplies/medical records etc around follow coloured lines on floor.
Patient exposure to other patients in the entryway.
Problems with bringing in new machinery to the new Stroke Department on the 2nd floor. New machines had to delivered by helicopter in after part of the ceiling was removed, the building had to be strengthened.
Security? Privacy?
THE TECHNOLOGICAL REVOLUTION IN THE ER
Revolution in radiology (Computers, then CT and MRI) has completely changed the way problems are diagnosed and the ability to diagnose. It is rare to have an MRI scanner in the ER.
Everything is digital now, even X-Ray no longer uses film.
Speed of information transfer 15 mins, can take longer, so radiologist will be present to look at the results as they appear on the screen as an initial check to make sure nothing serious is happening there and then.
In 1975, MGH installed the second CT scanner in the country (?), which was able to scan 4 slices per hour, and then took 1 hour to reconstruct the data. We saw the scanner processing and displaying enormous amounts of detail of the entire body in around 1 minute.
We thought about issues of power and also issues of server space and information storage. With its 6 CT scanners alone working 24/7, MGH must require extraordinary IT systems as well as the generators etc required by all hospitals. What happens if these go down?
The entire ER area has been rebuilt in the last 5 years in stages, (what complexities and compromise does an ongoing upgrade system like this entail
Future advances: biopsy– digital intervention, data/biological instead of cutting patients open to examine. How will this affect the ER of the future?
Anonymous at 12:28 PM
Friday, April 07, 2006
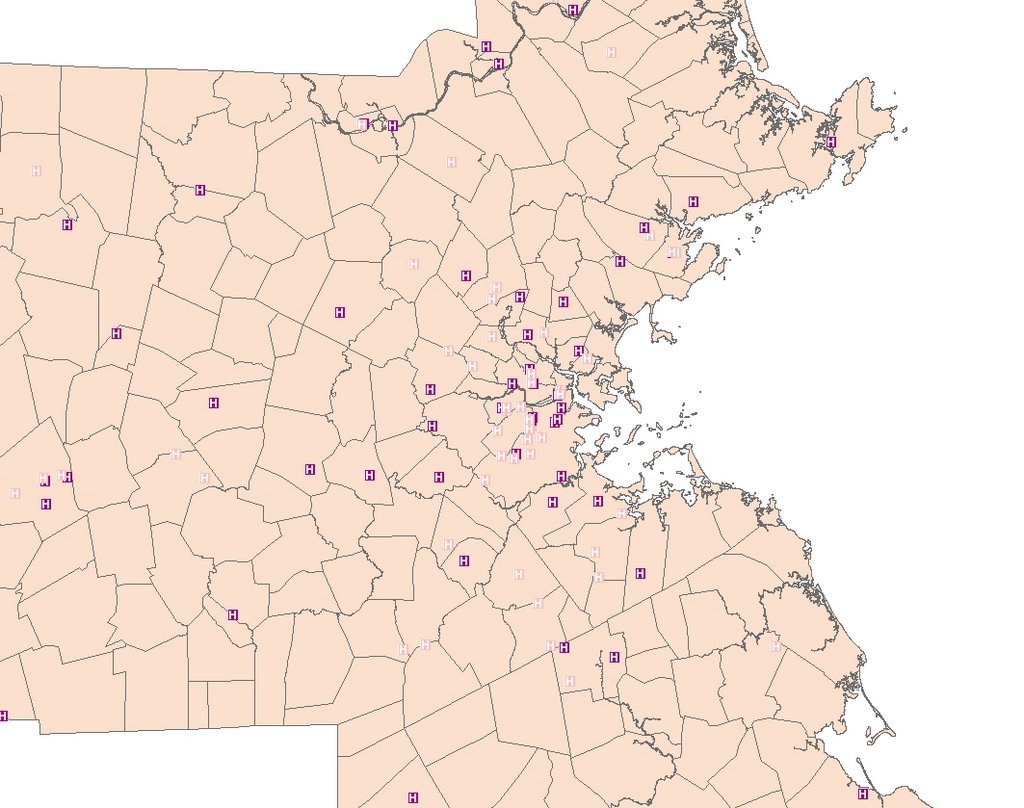
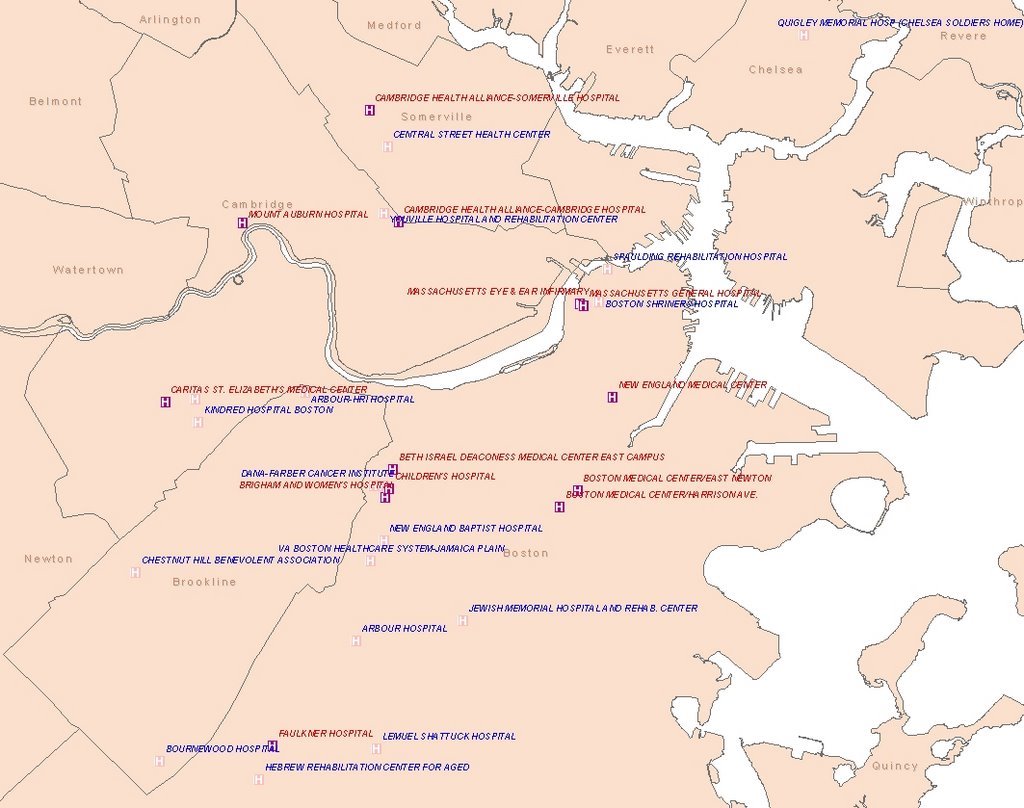
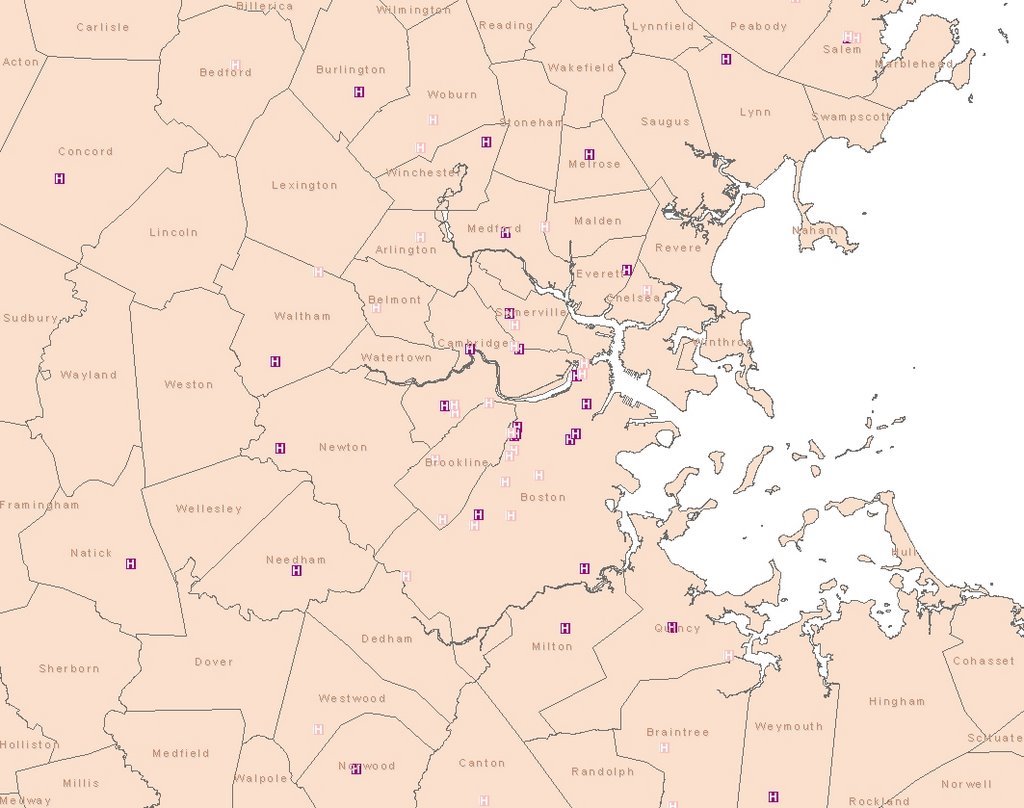
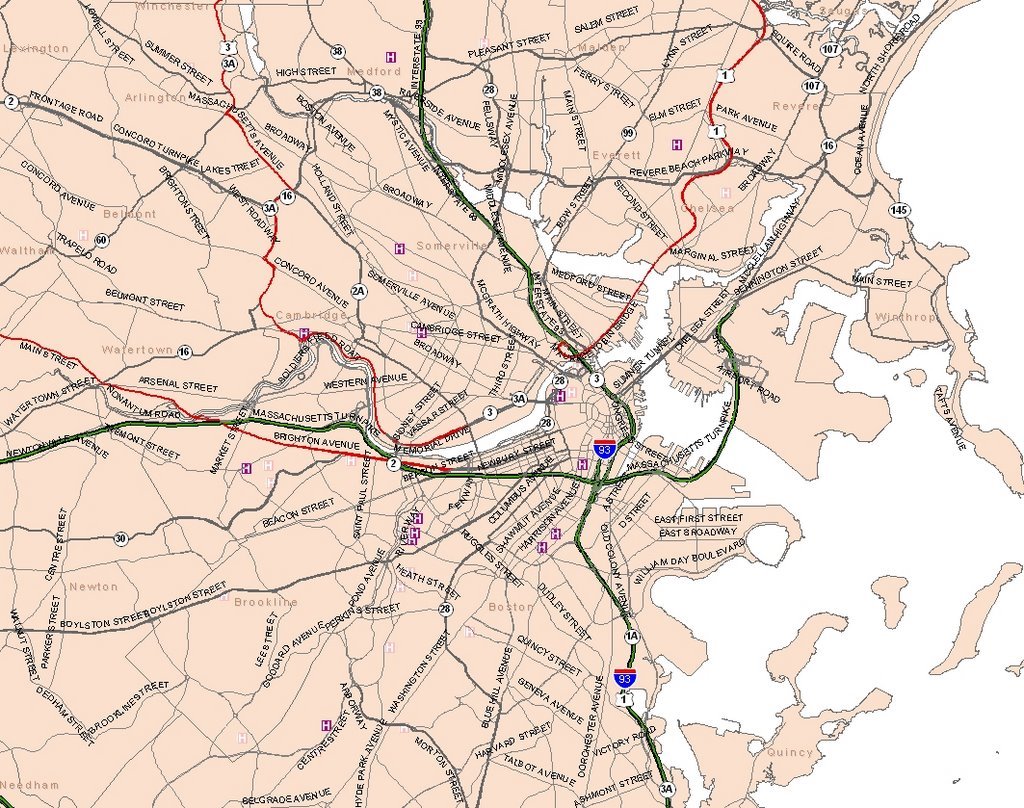
E.R. with GIS
We have researched on the location of emergency rooms and hospitals within MA
ER in MA

cati at 4:19 PM
Previous research
During the GSD product design research course, we researched and prototyped an integrated dropped ceiling.
cati at 4:18 PM
Research goal
The optimal goal of the class is to have a better understanding of the emergency rooms in US hospitals.
This blog will discuss our current research on E.R.
cati at 12:49 PM