« Home | information for construction process »
Thursday, April 13, 2006
Typologies and Spatial Analysis
In an attempt to understand how actual Emergency Rooms function we have consulted and visited with medical professionals immersed in the actual ER environment. While, admittedly, their design knowledge and opinions may be lacking, their understanding of the practical, actual, and utilitarian experiences can help us better understand the space. As designers it then becomes our task to decipher the design qualities that contribute to certain preferences.Interpretations of ER Descriptions
The following three hospitals are interpretations of spaces either described by medical workers or by site visits.
 University Hospital - New Jersey
University Hospital - New Jersey This first example is of University Hospital in New Jersey as described in a conversation with Ershad Elahi, a third year medical student at the New Jersey Medical School. The unique thing about this layout is that patients are immediately separated into two different categories: trauma and medical. This allows for a specialization of care that helps make the process smoother. While such a system does require essentially two distinct and complete staff, a well thought layout can utilize shared resources such as supplies and OR rooms.
 Rochester Emergency Facilities
Rochester Emergency FacilitiesThis second example, also described during a conversation with Ershad Elahi, is a layout of the Rochester Emergency Facilities. Unlike the linear example above, this plan is set up radially. The patient and OR rooms are placed at the perimeter of the plan to provide visual and circulatory access to the core of the building which is staffed with nurses and doctors. The supplies are central to the plan giving equal access to all those who might need it. As organized according to the conversation, it seems that this layout limits both expansion and access. However it does provide a fairly successful circulation scheme.
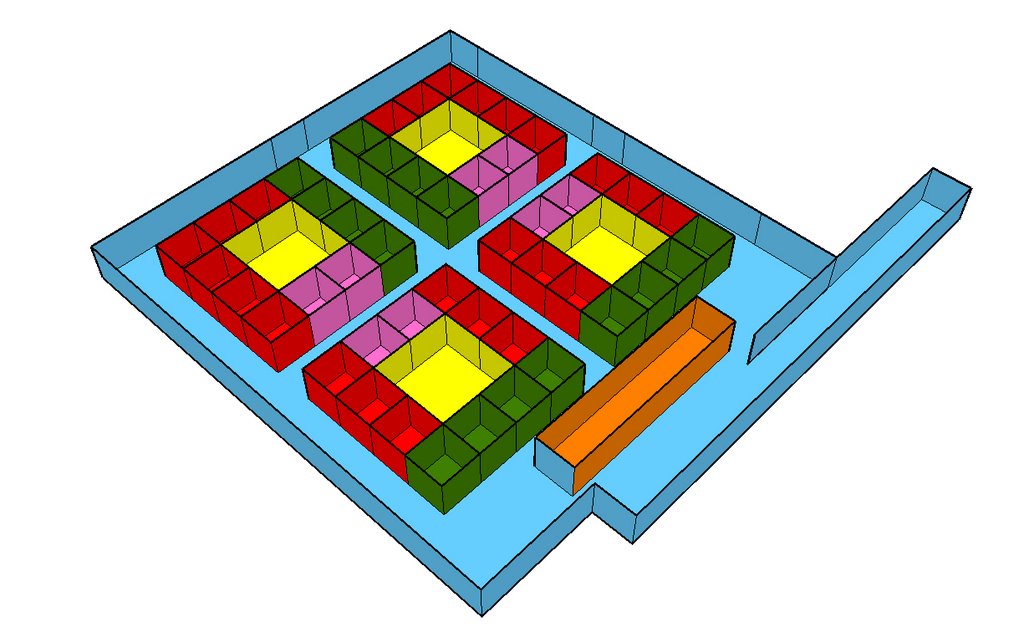 MGH: An Abstract Impression
MGH: An Abstract ImpressionOur visit to the emergency room at MGH was quick and disorienting, although quite educational. The space and layout was extremely difficult to understand in a short and furious tour through the facility. However, this layout explains the general impression of the space. This layout may be described as nodal, where particular functions and specialties pop up in concentrated cores of activity. Each core then becomes able to handle it's own nursing staff, doctors, technological support, specialty rooms, patient rooms and supplies. While as confusing to navigate as a McMansion suburban neighborhood, it is actually a very flexible system that allows for expansion in the long run.
Generic Hospital Layouts
Many of our sources often point generic plans to stress a point about trends in design and layout. The following three examples are just a sampling of the information that is out there on spatial analysis.
 Generic Layout 1
Generic Layout 1This layout, taken from Design Planning for Ambulatory Care Facilities shows a typical one way circulation system. The plan has a strong orientation that explains the process through the ER. Successful aspects of this design include access to the supplies and the nurses station from the important medical rooms (such as OR or Radiology). Some of the drawbacks of such a plan include the privacy issues associated with a large patient recovery room and the relative distance from things the further you make your way through the circulation diagram.
 Generic Layout 2
Generic Layout 2This plan, taken from Hospital Emergency Facilities uses some fairly typical layout strategies. First of all, it separates the patient rooms from the important activities in the hospital. In the buffer between these two you will find both supplies and the nurses/medical staff facilities. This buffer zone then allows for access of the staff and supplies both to the high resource side rooms and the patient rooms. Although the zones are clearly delineated, the segregation may be detrimental in the long run when it comes time for expansion. It might be nice to see this approach in a more "branched" layout.
 Generic Layout 3
Generic Layout 3Also from Hospital Emergency Facilities this layout separates more clearly the more important rooms of the ER from the rest of the program. This can be beneficial down the road because the integration of new technological or machine heavy equipment can be a hassle to integrate fully into a fixed plan. The peripheral quality of the more significant program will facilitate expansion and changes in medicine and technology. This is also a good example of clearly delineated entrances for walk-ins and ambulatory access. Another interesting thing about this layout is the mixing of nurses stations and supply closets. It seems that this then allows for greater access to more patients when such a system is not afforded (as in a radially scheme)
Typological Layouts
We have also been investigating generic strengths and weaknesses of hospital and ER typologies. The following three examples begin to stress some of the more pressing issues at hand when planning hospitals.
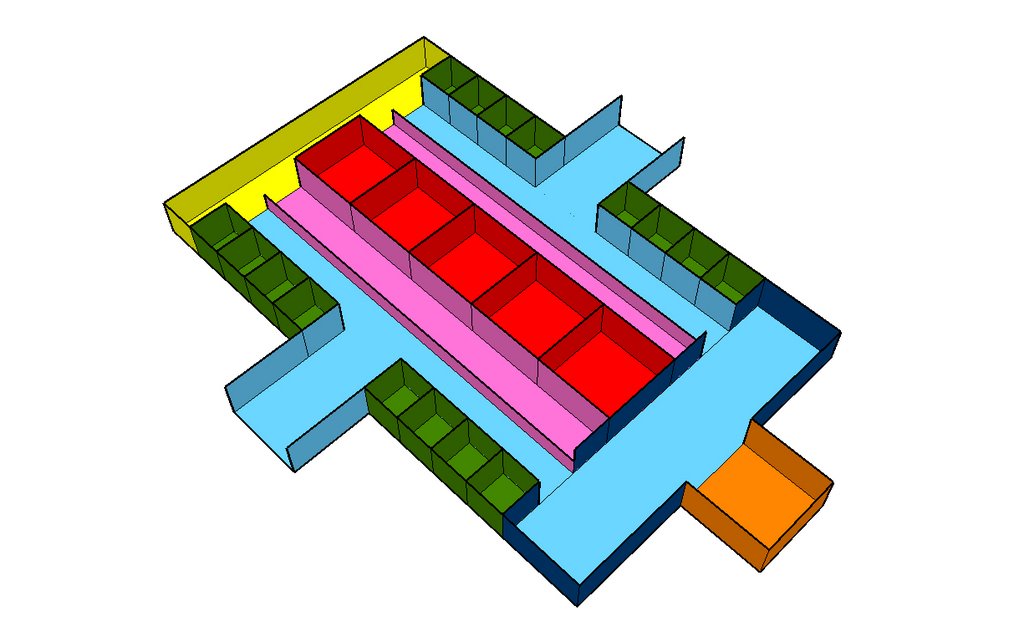
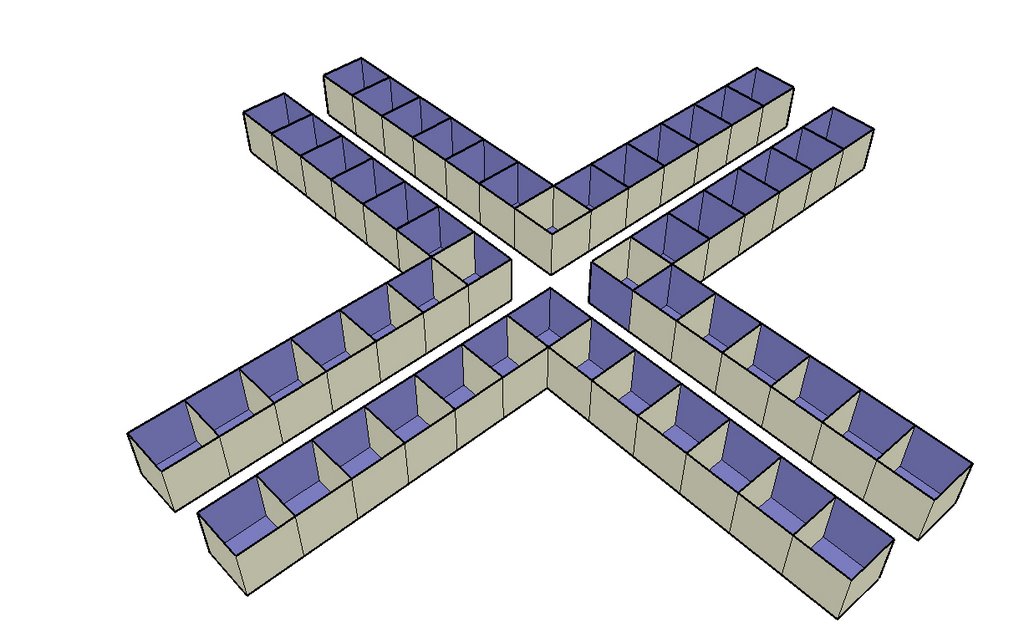 The Cross
The CrossA crucifix layout is strong in it's ability to distribute double-loaded program in the shortest walking distance. However it become very important to think about where shared resource are located. For instance, if the arms of the cross become specialized then it's difficult to determine the appropriate location for supplies, nurses stations, staff resting rooms, and ORs. However expansion, if there is room, is easier in an "appendage" plan because it takes less room to add on.
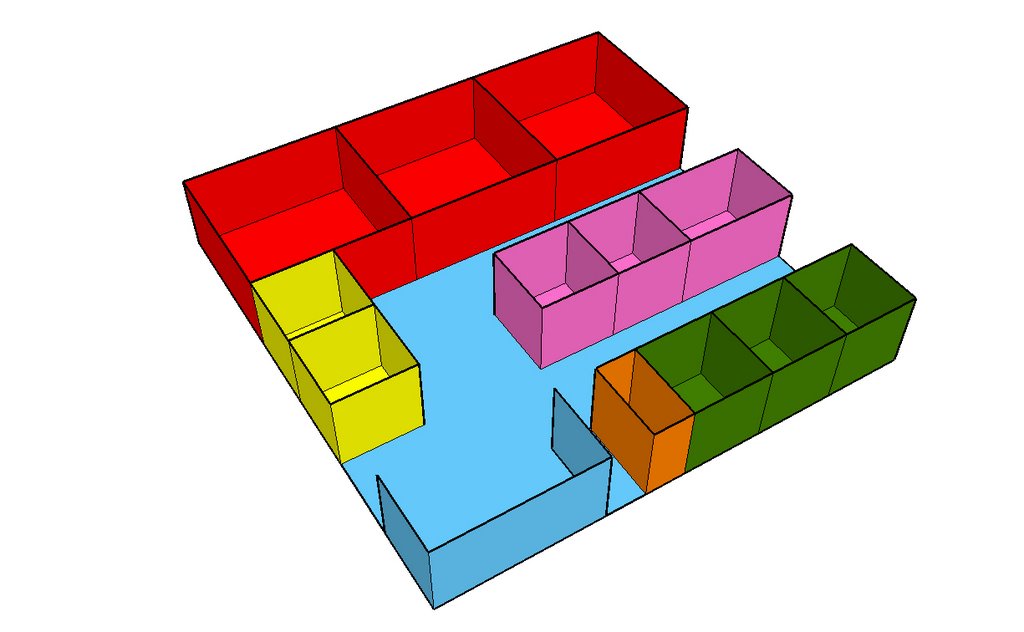
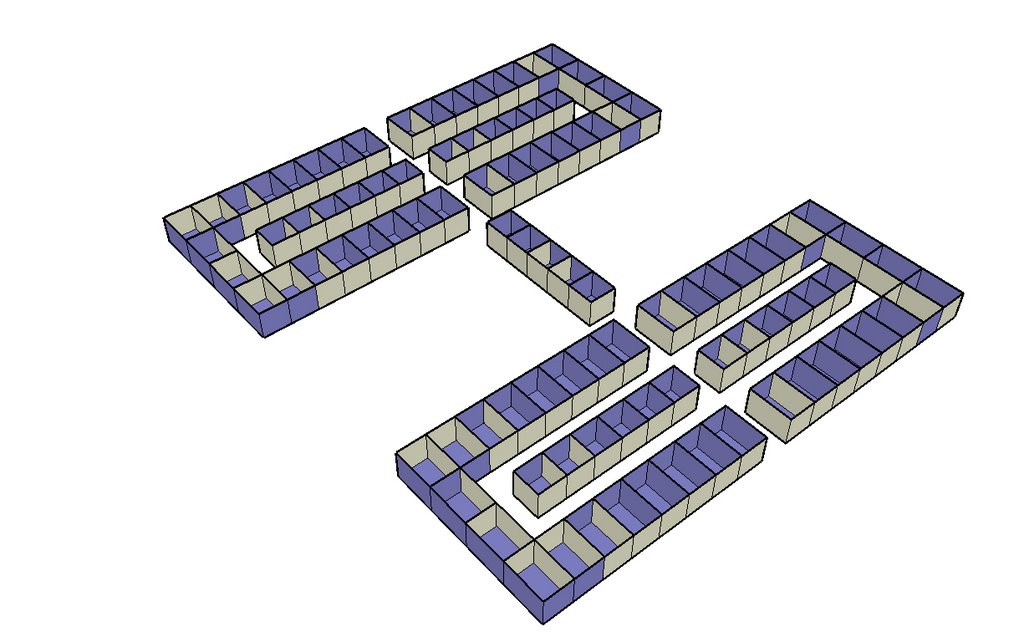 The Racetrack
The RacetrackThis plan is a good way to keep diverse programs in close proximity to each other. However, a drawback is that circulation quickly becomes long and disorienting. The strength in executing a plan like this would be to use the middle spaces as a transition space between one side of the hall and the other. This plan also allows for a certain degree of specialization.
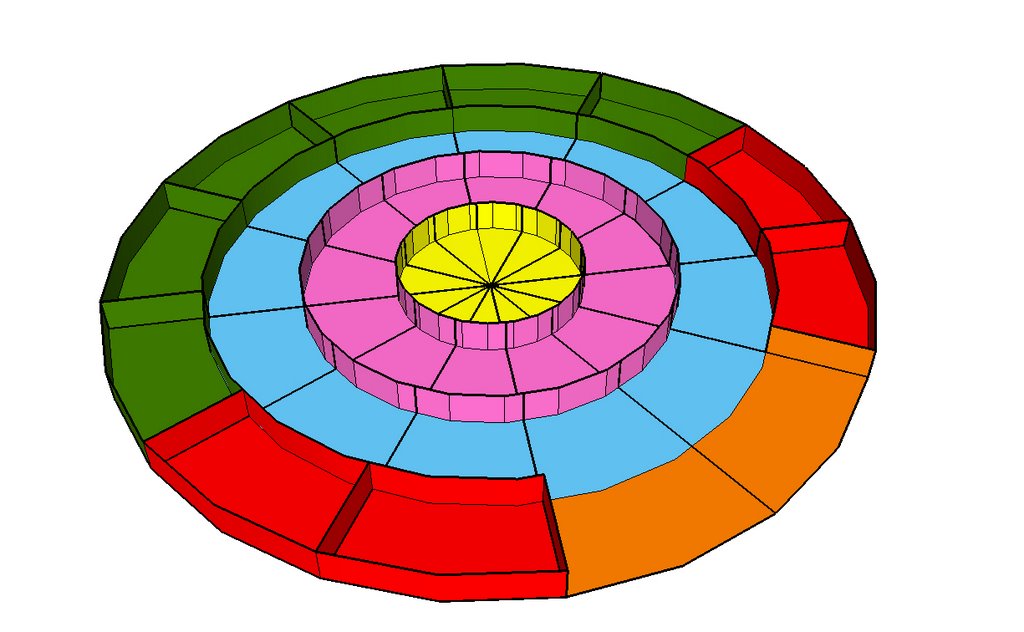
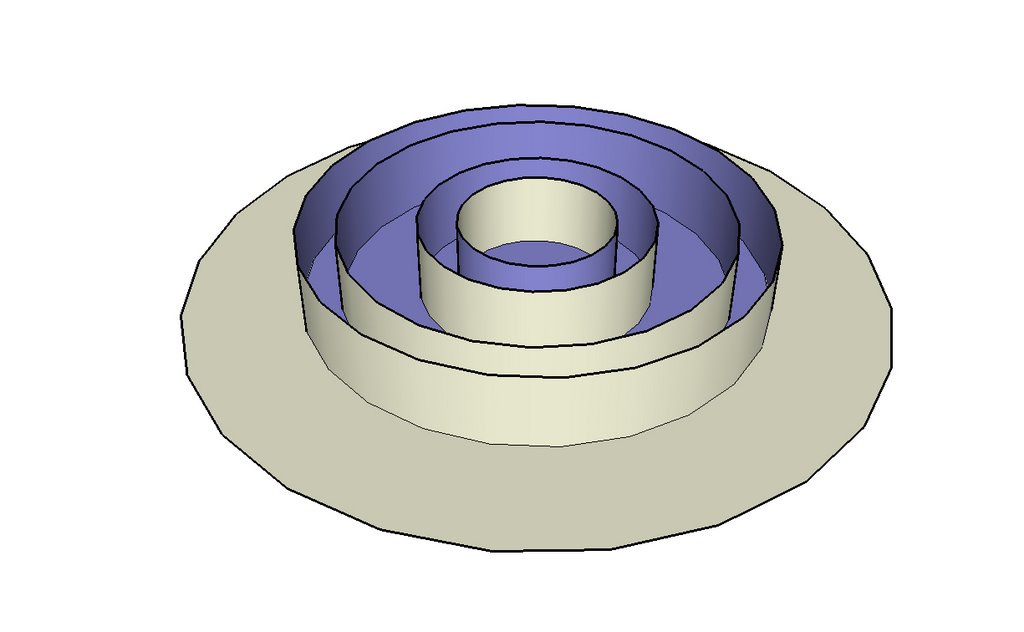 Radial
RadialThe radial plan, as seen earlier in an interview interpretation, is straightforward in it's approach to organizing circulation and programmatic overlap. The biggest downside of such a plan is that it is limited in capacity. To add another ring increases the built area exponentially and increase circulation difficulties. Ideally a radial plan would have supplies and medical staff located centrally so as to be easily distributed to the circumference. It is also interesting to note the varying types of private and public circulation, from the external car down to private medical staff.
Anonymous at 11:59 PM